
Many residents in Dallas reach this same point. Work still needs to get done. Kids still need rides. Bills still need to be paid. But anxiety, depression, trauma, drinking, pills, or drug use have started to make everyday life feel harder to hold together.
That's often where outpatient mental health treatment becomes the right conversation. It gives people a way to get real clinical support without automatically stepping away from home, school, family, or work. That matters because fear of disruption keeps many people stuck longer than they need to be. It's hard to ask for help when help sounds like putting life on pause.
Getting care is also far more common than many families realize. In 2023, approximately 59.2 million U.S. adults received treatment or counseling for their mental health within the past year, and the percentage of U.S. adults receiving any mental health treatment increased from 19.2% in 2019 to 21.6% in 2021, with especially strong growth among adults ages 18 to 44, according to Statista's summary of U.S. mental health treatment use.
Table of Contents
- When Your Life Needs Support Not Disruption
- Understanding Outpatient Mental Health Treatment
- Finding the Right Level of Outpatient Care in Dallas
- Integrating Mental Health and Addiction Recovery
- Your Path to Healing What to Expect
- Using Your Insurance for Treatment in Dallas Fort Worth
- Take the First Step Toward Wellness with Tru Dallas
When Your Life Needs Support Not Disruption
Someone in Dallas may already know something's wrong. Sleep is off. Mood is harder to manage. Alcohol or drugs may have shifted from a way to cope into a problem that's making everything worse. What often stops the next step isn't denial. It's the fear that treatment will blow up the routine that's still barely holding life together.

Outpatient mental health treatment exists for exactly that situation. It's designed for people who need more than occasional advice, but who may still be able to live at home and stay connected to daily responsibilities in Dallas, Euless, Irving, Plano, Frisco, or surrounding communities. The point isn't to ignore how serious symptoms can be. The point is to match treatment intensity to what is required.
Families also tend to underestimate how much untreated stress affects judgment, sleep, cravings, and conflict at home. Alongside formal treatment, some people also look for small lifestyle supports that may help the body settle, such as routines focused on sleep, movement, and lower cortisol levels. Those strategies can support recovery, but they don't replace clinical care when depression, anxiety, trauma, or substance use have started driving behavior.
Practical rule: If symptoms are interfering with safety, relationships, work, or substance use recovery, it's time to get a professional assessment rather than trying to push through alone.
The most reassuring part for many families is simple. Treatment doesn't have to mean disappearing from life. In many cases, it means building enough structure and support to stay in life more effectively.
Understanding Outpatient Mental Health Treatment
Outpatient care is easier to understand when it's compared to other medical treatment. A person goes to appointments, receives professional care, practices skills between visits, and returns home afterward. That's the basic model.
What outpatient care actually means
Outpatient mental health treatment refers to behavioral health services provided without an overnight stay. Depending on need, that may include individual therapy, group therapy, medication management, psychiatric follow-up, relapse-prevention work, or more structured programming several days a week.
For someone dealing with both mental health symptoms and substance use, outpatient care can be part of a broader recovery plan rather than a stand-alone service. It may follow detox, step down from a higher level of care, or begin as the first level of treatment if the person is medically stable and has a home environment that supports recovery.
A good outpatient program does not only schedule therapy and send people on their way. It evaluates risk, stability, motivation, symptom severity, relapse history, and practical pressures at home. Families looking for a fuller picture of how this fits into behavioral healthcare can review mental health treatment options in Dallas.
What outpatient care is not
Outpatient treatment is not a lighter version of care by default. It's a category with different levels inside it. Some people need a highly structured daytime schedule. Others need several focused sessions a week. Others do well with weekly therapy and medication check-ins.
It's also not the right fit for every situation. If someone is at immediate risk, medically unstable, actively withdrawing, unable to stop using safely, or too overwhelmed to function outside a controlled setting, a higher level of care is often more appropriate first.
Outpatient care works best when the clinical plan matches the person's actual level of instability, not the schedule they wish they could maintain.
There's also a practical side that families don't always consider. Access to care increasingly depends on clinician availability, and that includes flexible and virtual roles in the workforce. For people curious about how behavioral health staffing is evolving, resources about Remote Therapist Jobs offer some useful context for why outpatient options may look different than they did a few years ago.
The primary difference is that inpatient treatment provides a period of stabilization by removing an individual from their surroundings. Conversely, outpatient care supports recovery while the person remains in the environment where their symptoms, triggers, routines, and relationships exist.
Finding the Right Level of Outpatient Care in Dallas
Choosing the right level of care is where many families get stuck. They know help is needed, but they don't know whether that means a full day program, evening support, or weekly therapy. The answer depends less on labels and more on function. How impaired is daily life? How recent was detox or inpatient care? How stable is the home environment? How strong is the relapse risk?
Outpatient levels of care at a glance
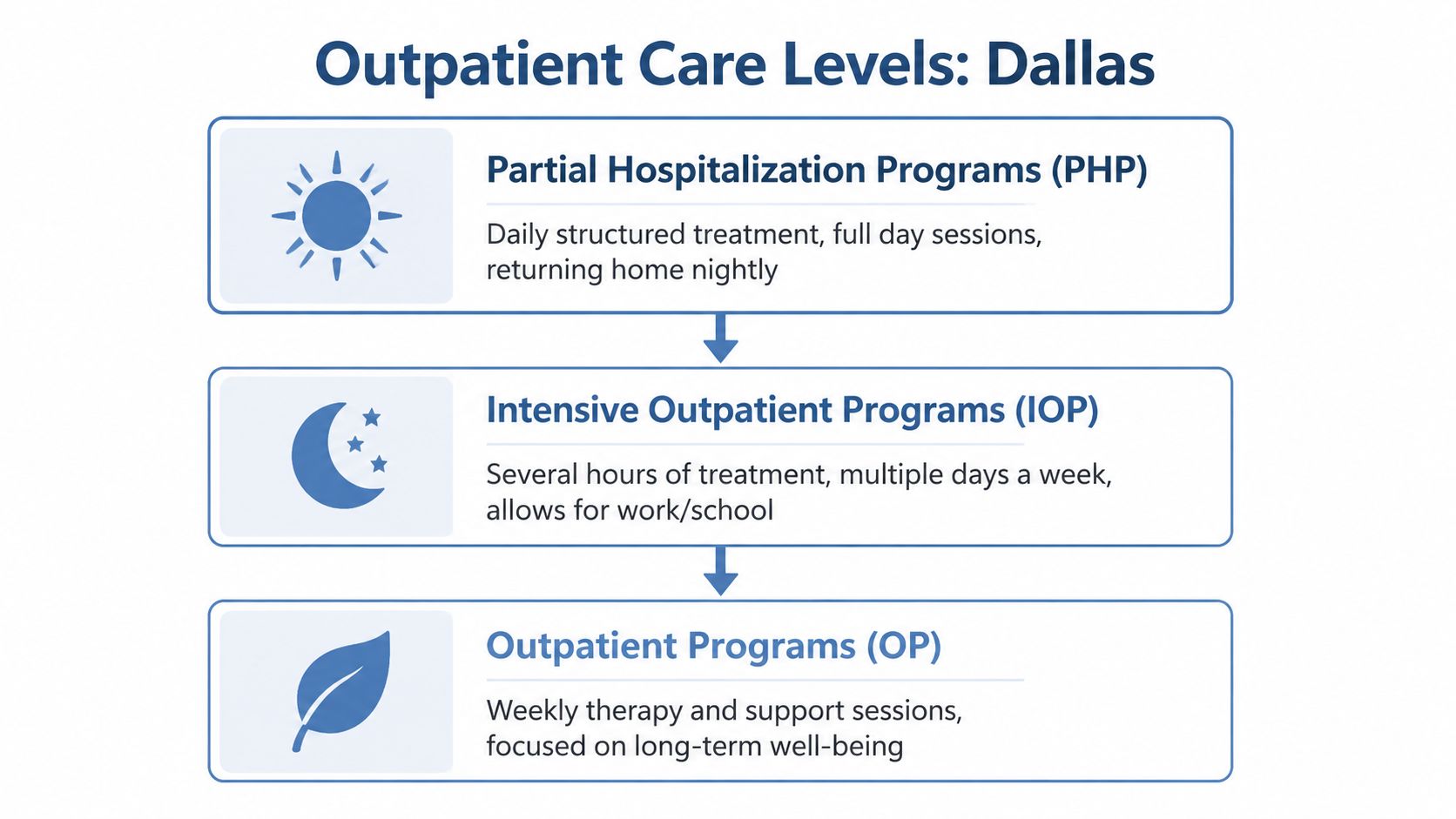
| Level of Care | Time Commitment | Best For | Therapy Structure |
|---|---|---|---|
| Partial Hospitalization Program (PHP) | Full day programming on treatment days, returning home at night | People who need strong structure and close clinical monitoring without overnight residential care | A mix of group therapy, individual sessions, psychiatric support, skills work, and recovery planning |
| Intensive Outpatient Program (IOP) | Several hours per day, multiple days each week | People stepping down from detox or inpatient care, or those who need more than weekly therapy but can still manage some daily responsibilities | Group therapy, individual therapy, relapse-prevention planning, family work, and medication support when needed |
| Outpatient Program (OP) | Usually weekly or otherwise scheduled appointments | People with more stability who need ongoing therapy, psychiatric follow-up, or long-term recovery support | Individual counseling, medication management, occasional groups, and continued care coordination |
When PHP makes sense
PHP is often the right fit when a person doesn't need overnight hospitalization, but clearly needs more than standard outpatient visits. This can include severe depression, escalating anxiety, unstable moods, high relapse vulnerability, or a difficult transition after detox.
A strong PHP gives the week structure. That matters because unstructured time often becomes the place where symptoms, avoidance, cravings, and conflict grow. In a Dallas-area setting, PHP can help a person stay connected to family while still receiving a clinically dense level of support during the day.
Signs that PHP may be appropriate include:
- Daily functioning has fallen off: Work performance, self-care, parenting, sleep, or basic routines are becoming hard to sustain.
- A recent higher level of care ended: The person is stable enough to go home, but not stable enough to rely on weekly visits.
- Relapse risk is high: Substance use urges, emotional volatility, or environmental triggers are still intense.
When IOP is the better fit
IOP is one of the most practical transition points in dual-diagnosis care. It gives people meaningful structure while leaving room for work, school, and family obligations. That balance is why it often becomes the bridge between intensive treatment and fully independent recovery.
For dual-diagnosis patients transitioning from detox, Intensive Outpatient Programs show 25% higher retention rates and a 40% reduction in relapse at 6 months compared to standard outpatient care, according to the 2025 meta-analysis referenced here. That matters because the weeks after detox are often the most deceptive. A person may feel better physically but still be highly vulnerable emotionally.
Families who want a deeper explanation of this level can review what intensive outpatient treatment involves.
A common mistake is stepping down too quickly because the crisis seems over. In dual-diagnosis treatment, the end of crisis is usually the beginning of skill-building.
IOP often works well when a person:
- Needs accountability: Multiple touchpoints each week help interrupt old patterns before they gather momentum.
- Is returning to normal life gradually: They're re-entering work, school, or parenting but still need structured support.
- Has both mental health and substance use concerns: Therapy can address the link between symptoms and use, rather than treating them as separate issues.
When routine outpatient works well
Routine outpatient treatment is best for people who have enough stability to benefit from less frequent care. That doesn't mean their symptoms are minor. It means they can use treatment effectively without needing heavy structure.
This level may include weekly therapy, medication management, trauma work, family sessions, or long-term relapse prevention. It's often where maintenance, deeper insight, and sustained behavior change happen.
For some Dallas residents, routine outpatient is the first step. For others, it's the right landing place after PHP or IOP. The clinical task isn't choosing the most intensive option. It's choosing the level that gives enough support to produce real movement.
Integrating Mental Health and Addiction Recovery
A common Dallas scenario looks like this. Someone stops drinking or using for a few days, feels clearer, and wants life to go back to normal. Then panic returns, sleep falls apart, irritability rises, or old trauma symptoms show up hard and fast. Within days, the substance use problem and the mental health problem are feeding each other again.
That is why dual-diagnosis care has to be connected from the start. Treating only the substance use leaves depression, anxiety, trauma, or bipolar symptoms in place. Treating only the psychiatric symptoms while active substance use continues can disrupt sleep, worsen judgment, complicate medication response, and make therapy less effective.

Why dual diagnosis treatment has to be connected
In practice, the question is rarely whether a person has one issue or the other. The clinical question is how the two problems interact day to day.
A person may drink to blunt social anxiety, then wake up with worse anxiety and more shame. Another may use stimulants to push through depression, then crash into deeper hopelessness. Someone in early opioid recovery may also have untreated trauma and a nervous system that stays on alert even when they want to be calm. If those links are missed, treatment plans become fragmented and relapse risk rises.
Structured outpatient care helps because the same team can watch patterns over time, adjust the plan, and respond before a setback turns into a full return to use. Research on outpatient retention and integrated care in PMC supports the value of consistent treatment and programs built for co-occurring disorders.
A connected plan usually includes a few core pieces:
- Mental health treatment: Therapy targets depression, anxiety, trauma symptoms, mood shifts, or chronic stress directly.
- Relapse prevention: Patients learn how cravings are affected by conflict, poor sleep, isolation, shame, and untreated psychiatric symptoms.
- Medication review: Prescribing decisions are made with recovery goals in mind, not in a separate silo.
- Family involvement: Loved ones get practical guidance about boundaries, support, and what warning signs to watch for.
How the transition from detox to outpatient should work
The handoffs between levels of care deserve close attention. I often tell families that detox answers one urgent question: can the person get through withdrawal safely? It does not answer the next question, which is how they will stay stable once the immediate physical crisis has passed.
For dual-diagnosis patients, that next step matters. A person leaving detox may still have severe anxiety, depressive symptoms, trauma reactions, sleep disruption, concentration problems, or strong cravings. Some need PHP because they require near-daily structure and close psychiatric follow-up. Others can step into IOP if they are stable enough to be home more often but still need several treatment contacts each week. Routine outpatient works better once symptoms, substance use risk, and daily functioning are steady enough to hold with less support.
The trade-off is straightforward. Stepping down too fast can leave a person with too little structure during the highest-risk period. Staying in a level of care that is more intensive than needed can strain work, school, childcare, and motivation. Good treatment planning weighs both realities instead of assuming more care is always better or less care is always easier.
Recovery is stronger when the handoff is warm, the discharge plan is specific, and the next appointment is scheduled before the current level ends.
That coordination is especially important for people in Dallas who are balancing treatment with jobs, parenting, transportation, court requirements, or school. Clear transitions reduce missed appointments, medication gaps, and the kind of confusion that can undo early progress.
Your Path to Healing What to Expect
Fear drops when the process becomes concrete. Many individuals do not require a sales pitch. They need to know what happens first, who they will talk to, what treatment days feel like, and whether anyone will notice if the plan is not working.
The first call and assessment
The process usually starts with a confidential phone conversation. That first contact is used to understand the immediate problem, current symptoms, substance use history, safety concerns, medications, and what level of care may fit best. If detox is needed first, that should be identified early rather than after an outpatient start fails.
The intake assessment then goes deeper. It looks at mental health history, prior treatment, relapse patterns, family dynamics, trauma exposure, home stability, and practical issues like transportation and scheduling. Good assessments don't just ask what diagnosis fits. They ask what is getting in the way of recovery right now.
What treatment looks like week to week
A treatment week may include individual therapy, group counseling, psychiatric follow-up, skills practice, and case coordination. Approaches often include cognitive behavioral therapy, dialectical behavior therapy, relapse-prevention work, and support for communication, boundaries, and emotional regulation.
Modern care should also be measurable. In data-driven outpatient mental health treatment, progress is measured at regular intervals using standardized tools such as the PHQ-9 for depression, allowing clinicians to adjust the plan in real time, as described in this overview of data-driven outpatient mental health treatment. That matters because symptoms change. The plan should change with them.
A strong week in treatment doesn't always feel dramatic. It often looks like:
- Clear goals: The person knows what symptoms or behaviors are being targeted.
- Active practice: Skills learned in session are tested in daily life between appointments.
- Review and adjustment: If something isn't working, clinicians respond instead of repeating the same plan.
- Support without judgment: The person can report urges, setbacks, or worsening symptoms openly.
The best treatment plans are collaborative. They don't rely on guesswork, and they don't treat silence as progress.
For many families, that transparency is what finally makes care feel manageable rather than mysterious.
Using Your Insurance for Treatment in Dallas Fort Worth
Cost is one of the first reasons families delay care. Confusion is another. Many people aren't sure whether outpatient mental health treatment, addiction treatment, detox, psychiatric visits, or medication-assisted treatment are covered under their plan, and they often give up before getting a clear answer.
What families usually need to know first
Many PPO plans provide benefits for behavioral health treatment, but coverage details can vary. The key questions usually involve deductibles, out-of-pocket responsibility, prior authorization, and whether a specific level of care is covered based on medical necessity.
Access is still a real barrier. National data shows that 28% of U.S. adults with any mental illness receive no treatment, and provider content often doesn't help families manage the financial side of care, according to the Behavioral Health Safety Net information cited here. In Dallas-Fort Worth, families often need straightforward help interpreting benefits, not more jargon.
How to make the process easier
A useful starting point is to gather the insurance card, current medications, and a short summary of what's happening now. That might include recent detox, active substance use, panic attacks, depression, missed work, or prior treatment attempts. Those details help determine both clinical fit and likely insurance pathways.
Families also benefit from learning the basics before they call. This guide on whether insurance covers drug rehab can help clarify common terms and what to expect during benefit review.
A practical admissions team should be able to help with:
- Benefit verification: Confirming whether outpatient, detox, or related services may be covered.
- Level-of-care questions: Explaining why PHP, IOP, or routine outpatient might be approved differently.
- Next-step planning: Helping the family understand what documentation or clinical evaluation may be needed.
The right conversation can remove a major barrier. Families shouldn't have to decode insurance language alone while also trying to keep a loved one safe.
Take the First Step Toward Wellness with Tru Dallas
A common call starts the same way. Someone has finished detox or knows they probably need it, but they do not know what comes after. The family is asking whether PHP is too much, whether IOP is enough, or whether weekly therapy can realistically hold things together when both mental health symptoms and substance use are in the picture.
The right next step is a clinical assessment that looks at the full situation, not just one diagnosis. In practice, that means reviewing safety concerns, withdrawal risk, current substance use, psychiatric symptoms, daily functioning, prior treatment, medications, and support at home. Those details help determine whether a person should start with detox, step into PHP after stabilization, begin with IOP, or enter routine outpatient care with a clear follow-up plan.
Good treatment planning also accounts for transitions. A person leaving detox may need more structure for a period of time, especially if cravings, mood instability, trauma symptoms, or relapse risk are still high. Someone in PHP may improve enough to step down to IOP, then continue with outpatient therapy and medication management. That progression often works best when each level of care is connected and the handoff is clear.
Early contact helps preserve options. In Dallas, Fort Worth, Euless, Irving, Plano, and nearby communities, people usually have more flexibility when they reach out before the situation becomes an emergency.
If you are trying to sort out depression, anxiety, trauma, alcohol use, drug use, or a dual-diagnosis situation, a confidential conversation can turn confusion into a practical plan.
Tru Dallas Detox & Recovery Center provides confidential guidance for people who need help sorting out detox, dual diagnosis treatment, outpatient options, and insurance questions. A simple conversation can clarify the appropriate level of care and the next step.