The call usually comes after a hard night. A spouse has been up listening for breathing. An adult child has watched shaking, sweating, panic, or confusion get worse by the hour. The person drinking says they want to stop, but they're terrified of what happens next.
That fear makes sense. Alcohol withdrawal can turn dangerous quickly, and trying to manage it alone often goes badly. A librium taper alcohol withdrawal plan gives the body a controlled way through detox, with medication, monitoring, and adjustments based on real symptoms instead of guesswork. For anyone wondering what safe alcohol detox looks like in the Dallas area, this guide explains the process in plain language and outlines why safe alcohol detox steps should always include medical oversight.
Table of Contents
- Navigating Alcohol Withdrawal with a Safe Medical Taper
- Why Librium Is a Gold Standard for Alcohol Detox
- Understanding Librium Tapering Schedules and Protocols
- Critical Safety Warnings and Professional Monitoring
- Choosing the Right Detox Setting in Dallas
- Beyond the Taper Your Next Steps to Recovery in Dallas
- Frequently Asked Questions About Librium Tapers
Navigating Alcohol Withdrawal with a Safe Medical Taper
Stopping alcohol after heavy or prolonged use can feel like stepping into the unknown. Many people expect discomfort. What they don't expect is how fast symptoms can escalate, or how hard it is to judge whether the situation is still manageable at home.
A medical taper changes that. Instead of waiting for symptoms to spike and reacting late, clinicians use medication in a structured way to reduce withdrawal stress on the brain and body. The purpose isn't to replace one problem with another. It's to prevent a dangerous swing in the nervous system while the body clears alcohol.
What a safe start usually looks like
A safe detox plan begins with assessment. The team looks at recent drinking, prior withdrawals, current symptoms, medical history, medications, and mental health concerns. That information determines whether the person needs inpatient monitoring, a symptom-based taper, or another level of support.
Then the taper begins under observation. Staff monitor how the person is doing, watch for red flags, and adjust treatment based on actual clinical signs rather than hope.
Practical rule: If a person has a history of intense withdrawal, confusion, seizures, severe anxiety, or unstable medical symptoms, home detox isn't a reasonable gamble.
For families in Dallas, Highland Park, Oak Lawn, Plano, Irving, Arlington, and nearby communities, the biggest relief often comes from knowing there's a plan. Alcohol withdrawal feels chaotic when no one is in charge of it. It becomes more manageable when a medical team takes over symptom tracking, medication decisions, hydration support, and next-step planning.
Why people do better with structure
The first goal is safety. The second is steadiness. A good taper avoids the cycle of waiting until symptoms become unbearable, then trying to catch up.
That's why medically supervised detox often feels calmer than people expect. The environment is structured. Monitoring is consistent. The person isn't left deciding alone whether shaking, sweating, panic, or rising agitation is “normal enough” to push through.
Why Librium Is a Gold Standard for Alcohol Detox

A family brings someone into detox after a night of shaking, sweating, panic, and no sleep. The question they usually ask is simple: why this medication?
Librium, or chlordiazepoxide, has stayed a standard medication in alcohol detox for one practical reason. It gives many patients steadier coverage during the period when withdrawal symptoms can intensify fast. That longer-lasting effect can reduce the sharp ups and downs that make alcohol withdrawal harder to control and more dangerous to treat casually at home.
People often hear “benzodiazepine” and assume the medication creates a second problem. In a detox setting, the goal is short-term stabilization. Librium is used in a controlled way, then reduced as the patient moves through withdrawal under medical supervision.
For readers comparing options, this overview of medications used in alcohol withdrawal treatment explains why one medication may fit one patient better than another.
What Librium does during withdrawal
Alcohol withdrawal pushes the nervous system into a hyperactive state. Patients may develop tremor, anxiety, sweating, nausea, insomnia, agitation, and rising blood pressure or heart rate. In severe cases, the risks include seizures, hallucinations, and delirium tremens.
Librium helps slow that overactivation. In real clinical practice, the value is not just that it reduces symptoms. It can also create a more stable treatment window so the team can reassess the patient, watch for complications, and decide whether a symptom-triggered approach or a fixed-dose taper makes better sense for that specific case.
That distinction matters. A patient with predictable symptoms, reliable reporting, and close observation may do well with medication given in response to withdrawal severity. A patient with a history of severe withdrawal, limited ability to report symptoms clearly, co-occurring medical issues, or a higher seizure risk may need the structure of a fixed-dose plan. Librium is often chosen because its long duration gives clinicians room to make those adjustments more safely than a shorter-acting option would.
Why its longer action matters
Shorter-acting medications can wear off faster and leave less margin for error if symptoms rebound between doses. Librium tends to produce a smoother decline in medication levels over time. That is one reason many detox clinicians still trust it for alcohol withdrawal.
Patients and families usually feel that difference as fewer abrupt swings. Clinicians see it as better symptom buffering while the body recalibrates.
A smoother medication curve does not remove risk. It reduces some of the volatility, but the patient still needs monitoring for oversedation, confusion, falls, breathing concerns, and symptoms that break through despite treatment.
In Dallas detox settings, the primary challenge is rarely the medication alone. It is matching the medication plan to the patient in front of us. Someone who is older, medically fragile, taking other sedating medications, or arriving after repeated withdrawal episodes may need a very different Librium strategy than a younger patient with milder symptoms. That is why individualized medical oversight in a facility such as Tru Dallas matters. The safest use of Librium depends on choosing the right taper method, adjusting it as symptoms change, and watching closely enough to catch problems early.
Understanding Librium Tapering Schedules and Protocols
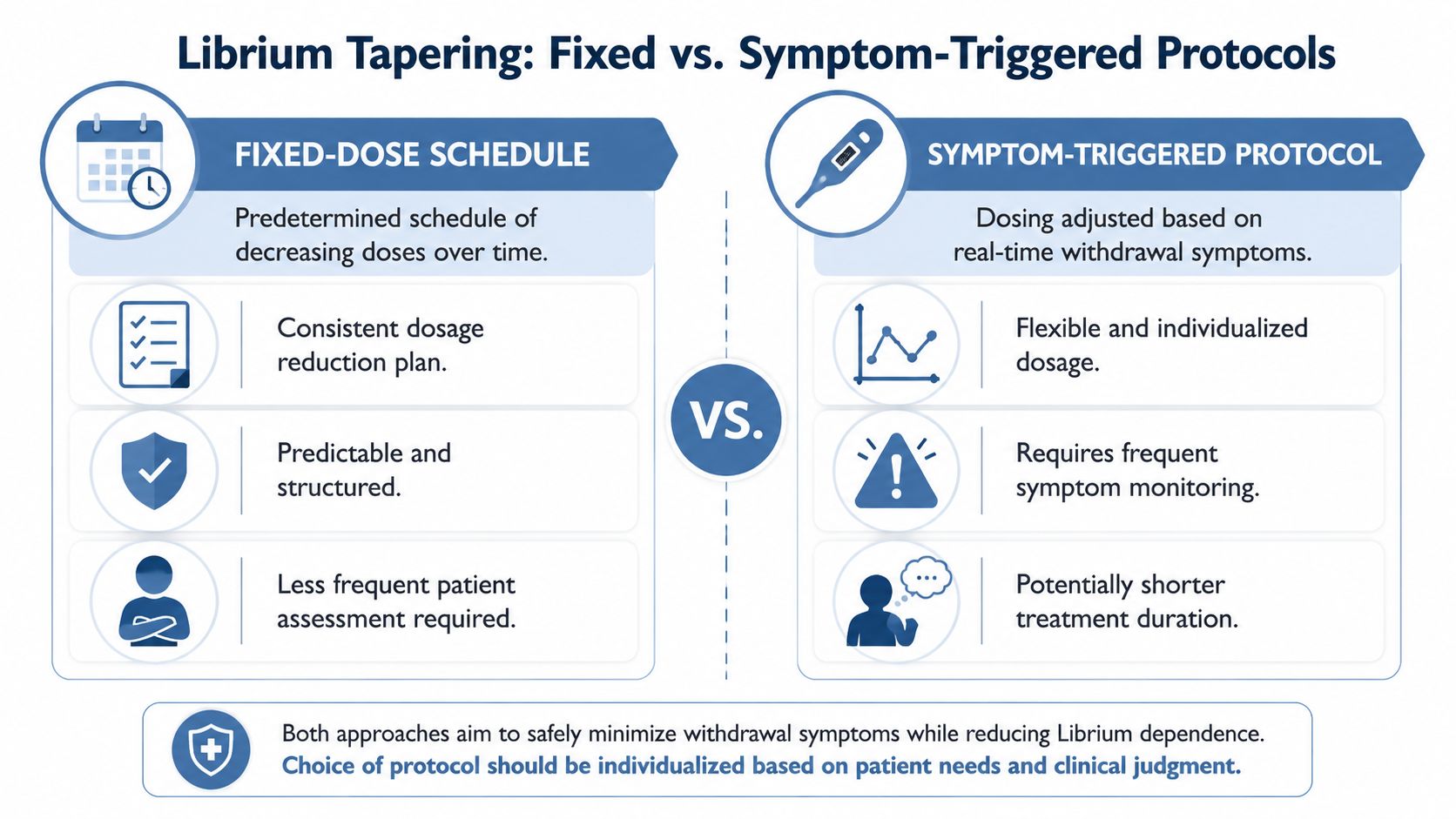
A family in Dallas may call us after a rough night and ask what the Librium taper will look like. The honest answer is that there is no single schedule that fits every patient. The first decision is whether the patient is safer on a fixed-dose protocol or a symptom-triggered protocol. That choice affects dose timing, reassessment frequency, and how quickly the team can adjust if withdrawal changes course.
In a supervised detox setting, clinicians often use the CIWA-Ar scale as one part of that decision. It helps organize symptoms such as tremor, sweating, agitation, nausea, and sensory disturbance. The score matters, but bedside judgment matters just as much. I have seen patients who score modestly but look medically fragile, and others who score high because of panic, sleep deprivation, or another psychiatric issue layered on top of withdrawal.
How fixed-dose tapers work
A fixed-dose taper gives Librium on a preset schedule, then reduces the dose in planned steps. This approach gives structure. It can be the safer choice for patients with a history of severe withdrawal, unreliable symptom reporting, cognitive impairment, or a situation where repeated scoring may not reflect what is really happening.
Families often find this method easier to follow because the plan is clear from the start. Clinically, the trade-off is that a preset schedule can give too much medication to one patient and not enough to another if the course changes faster than expected.
Fixed-dose protocols are often considered when:
- Withdrawal risk is higher: Prior seizures, delirium tremens, or repeated detox episodes raise concern for rapid escalation.
- Symptom reporting is limited: Confusion, language barriers, poor insight, or co-occurring psychiatric symptoms can make symptom scores less reliable.
- Monitoring is less continuous: A structured schedule may be more practical when the patient cannot be reassessed as frequently as a symptom-triggered plan requires.
How symptom-triggered tapers work
A symptom-triggered protocol gives medication in response to current withdrawal signs rather than by the clock alone. If symptoms stay mild, the patient may need less Librium overall. If symptoms increase, the team can respond quickly with additional dosing and closer observation.
This method can work well in the right setting, but only when assessments are frequent and consistent. The person doing the scoring has to know alcohol withdrawal well enough to spot the patient whose condition is worsening even before the number fully reflects it. That is one reason symptom-triggered detox is better suited to a medical setting than an unsupervised home plan.
Why this choice matters so much
The fixed-dose versus symptom-triggered decision is often treated like a small detail. It is not. It is one of the main safety decisions in alcohol detox.
A symptom-triggered plan may reduce unnecessary medication for a stable patient. A fixed-dose plan may offer better protection for someone with a more dangerous withdrawal history. Neither approach is automatically better. The better approach is the one that matches the patient in front of the team.
In a Dallas facility such as Tru Dallas, that means looking beyond the checklist. Age, liver function, other sedating medications, past withdrawals, current vital signs, and co-occurring mental health symptoms all affect protocol choice. Some patients also need front-loading or a faster escalation of care because their withdrawal is building despite treatment.
For worried families, this is the point to hold onto. A safe librium taper alcohol withdrawal plan is not just about getting the drug and waiting several days. It is about choosing the right protocol, reassessing often, and changing course early if the patient is drifting toward trouble.
Critical Safety Warnings and Professional Monitoring

A common Dallas detox call starts the same way. A family says their loved one is shaky, scared, and has taken the first Librium dose, so they hope the hard part is over. Sometimes it is not. Alcohol withdrawal can turn fast, and a person who seems only anxious in the morning can be confused, hallucinating, or medically unstable by evening.
That is why monitoring matters as much as the prescription itself.
What can go wrong without supervision
Alcohol withdrawal is not just a comfort issue. It can involve severe agitation, vomiting, dehydration, high blood pressure, disorientation, hallucinations, and seizures. Families should not try to sort out those changes at home, especially when sleep deprivation, panic, or other substances are clouding the picture.
Librium also has to be watched closely. A patient may become overly sedated, keep worsening despite treatment, or show symptoms that are partly driven by stimulant use, opioid use, liver impairment, or an underlying psychiatric condition. In practice, the danger is not only too little medication. Too much medication in the wrong patient can be just as unsafe.
These warning signs need immediate medical evaluation:
- Confusion or disorientation: The person cannot follow a simple conversation or does not know where they are.
- Seizure activity or collapse: Any seizure-like event is a medical emergency.
- Hallucinations or extreme agitation: Seeing or hearing things that are not there, or becoming severely combative, raises concern for complicated withdrawal.
- Trouble breathing or marked oversedation: This risk is higher if alcohol, sleep medications, opioids, or other sedatives are involved.
- Chest pain, fainting, or unstable vital signs: These symptoms should not be watched at home to see if they pass.
What professional monitoring actually looks like
A medically supervised detox unit does much more than dispense scheduled doses. Staff check vital signs, level of consciousness, hydration, intake, orientation, and response to each dose over time. They also watch for the less obvious shift, the patient whose score looks manageable but whose speech, gait, or attention is starting to deteriorate.
That matters most in the exact gray area families usually miss. The team is not only treating withdrawal. The team is deciding whether the current protocol still fits the patient safely.
This is especially important when mental health symptoms are present. Anxiety, panic, trauma reactions, bipolar symptoms, and severe depression can all change how withdrawal appears at the bedside. A symptom-triggered approach can work well for the right patient, but it depends on accurate scoring and frequent reassessment. If psychiatric symptoms distort the picture, a fixed-dose plan or a higher level of observation may be the safer choice.
I tell families this often. Protocols are tools, not autopilot.
In a Dallas facility such as Tru Dallas, good monitoring means the plan can change early. A patient who becomes too sleepy may need dose adjustments. A patient whose tremor, blood pressure, and confusion are building despite Librium may need a different taper structure, additional medical support, or transfer to a hospital level of care. Families who want a clearer picture of that process can review what medically supervised detox in Dallas looks like.
Transport planning matters too, especially if someone is deteriorating away from home or while traveling. Families who need to understand higher-acuity transfer options can review this emergency medical transport guide for families.
The safest message is also the simplest. If a person is withdrawing from alcohol and the symptoms are changing quickly, do not rely on guesswork, internet advice, or yesterday's dosing plan. Get medical eyes on them.
Choosing the Right Detox Setting in Dallas
At 10 p.m., a family member notices that their loved one is shaking more, sweating through clothes, and insisting they can manage detox at home because they already have Librium. That is the moment setting matters. The medication helps, but the safety of the taper depends on where it is given, how closely the person is watched, and whether the dosing plan matches the withdrawal pattern in real time.
The choice is not merely inpatient versus outpatient. In practice, the more important question is whether the patient is a good fit for a symptom-triggered taper or needs a fixed-dose schedule with closer observation. That decision can change quickly. A person who seems appropriate for a lighter-touch plan in the morning may look very different by evening if confusion, vomiting, rising blood pressure, or poor oral intake develop.
Anyone in Dallas, Euless, Grapevine, Fort Worth, Richardson, or the broader DFW area who wants a clearer picture of admission, monitoring, and daily medical care can review what medically supervised detox in Dallas looks like.
A practical way to decide
Outpatient detox can work for a narrow group of patients. They usually have mild and stable symptoms, a dependable sober adult at home, transportation, reliable follow-up, and no recent history of severe withdrawal. They also need to report changes accurately and take medication exactly as directed.
Many patients do not meet that standard. Some have had prior withdrawal complications. Some are medically frail, highly anxious, sleep deprived, or dealing with depression, trauma symptoms, or bipolar disorder that can blur the picture. In those cases, the setting has to support fast reassessment. That is especially true when clinicians are deciding between symptom-triggered dosing and a fixed-dose taper, because the safer option depends on what the patient is doing at the bedside, not what the plan looked like on paper.
Transport can become part of the safety decision too. When a medically vulnerable person cannot travel independently, families often need to think through supervision and transfer logistics before symptoms worsen. This emergency medical transport guide for families can help with that planning.
Inpatient vs outpatient detox
| Consideration | Inpatient Detox (e.g., Tru Dallas) | Outpatient Taper |
|---|---|---|
| Taper structure | Better for patients who may need a switch between symptom-triggered dosing and a fixed-dose schedule | Better only when the taper plan is unlikely to need rapid changes |
| Withdrawal course | Better suited for symptoms that may intensify over hours, not days | Better suited for milder, more predictable withdrawal |
| Monitoring | Ongoing observation with prompt response if sedation or worsening symptoms appear | Depends on scheduled visits and accurate reporting from the patient and family |
| Medication adjustments | Clinicians can change dosing the same day based on current findings | Changes may be delayed if the patient worsens between check-ins |
| Home setting | Helpful when home is unstable, unsafe, or lacks sober support | Requires a calm home, clear supervision, and dependable follow-through |
| Mental health complexity | Better when psychiatric symptoms may complicate assessment | Harder when anxiety, depression, trauma, or bipolar symptoms muddy the withdrawal picture |
| Escalation of care | Faster transfer to a higher level of medical support if needed | Greater risk if serious symptoms develop away from care |
Tru Dallas Detox & Recovery Center is one local option for patients who need medically supervised detox, close monitoring, and treatment planning that also accounts for co-occurring mental health concerns.
A simple rule helps families make the call. If you would not feel safe watching the person at home through the night, an outpatient Librium taper is probably the wrong setting.
Beyond the Taper Your Next Steps to Recovery in Dallas

A successful taper gets someone through withdrawal. It doesn't answer the harder question of how they'll stay well after the acute crisis passes. That's where many relapses begin. The physical symptoms ease, but the stressors, cravings, habits, and mental health drivers are still there.
Detox is the first step not the whole treatment plan
After alcohol detox, patients often need a structured next level of care. That may include residential treatment, therapy, psychiatric support, relapse-prevention planning, medication management, and a clear discharge plan. The right combination depends on the person's history, support system, and mental health needs.
What tends to help most after detox includes:
- Consistent therapy: Individual counseling helps identify what drives drinking, not just what happens during withdrawal.
- Group support: Patients benefit from hearing how others handle cravings, shame, stress, and family strain.
- Dual diagnosis care: If depression, anxiety, or bipolar symptoms are present, those issues need active treatment too.
- Aftercare planning: Recovery is more stable when the patient leaves with appointments, routines, and practical support already arranged.
What helps after withdrawal settles
Families often focus on surviving the first days, which is understandable. But recovery becomes more durable when treatment also includes stress management, sleep restoration, and healthier ways to regulate the nervous system. For some people, supportive wellness practices can complement formal treatment. This article on compare stress relief modalities offers a useful example of how people think through calming practices after the acute stage, though it should never replace clinical addiction care.
The goal after detox isn't to return to “normal” as fast as possible. It's to build a life that doesn't keep pushing the person back toward alcohol.
For someone in Dallas who's finally ready, the next step should happen quickly. Waiting until motivation fades rarely works. A confidential assessment, insurance verification, and a same-day conversation about detox can turn a crisis moment into a treatment plan.
Frequently Asked Questions About Librium Tapers
A common call goes like this: a spouse says their loved one stopped drinking, started shaking, and wants to take Librium at home and “wait it out.” That is the moment when the plan matters. The medication matters too, but the bigger safety question is whether the person needs a fixed-dose taper, a symptom-triggered protocol, or a higher level of care altogether.
Can someone detox from alcohol at home with Librium
Sometimes, but only in carefully selected cases with medical guidance and reliable follow-up. Librium can reduce withdrawal symptoms, but it does not make alcohol withdrawal predictable. Symptoms can intensify quickly, especially in people with prior severe withdrawal, seizures, heavy daily alcohol use, older age, other sedating drugs on board, or active medical and psychiatric problems.
Home detox becomes much riskier when there is confusion, rising blood pressure, persistent vomiting, hallucinations, poor hydration, or no dependable adult who can monitor the person and call for help.
How long does a Librium taper last for alcohol withdrawal
Many Librium tapers last several days. Some are shorter. Some need to be adjusted along the way.
The right duration depends on what the patient is doing in real time, not on a schedule copied from the internet. In practice, the choice between symptom-triggered dosing and a fixed-dose taper often shapes the timeline. Symptom-triggered care can use less medication when trained staff reassess frequently and the patient can report symptoms clearly. A fixed-dose taper may be safer when symptoms are expected to escalate, the history is concerning, or the patient cannot give reliable feedback.
Is symptom triggered always better than fixed dose
No. Each approach has strengths and limits.
Symptom-triggered protocols work well in a supervised setting where staff can check the patient often, score withdrawal accurately, and respond fast if the picture changes. Fixed-dose tapers offer more structure and can be the better choice when someone has a history of severe withdrawal, significant anxiety that muddies symptom scoring, cognitive impairment, polysubstance use, or limited ability to communicate clearly.
This is one of the most overlooked parts of detox planning. The safer protocol is the one that matches the patient in front of you, not the one that sounds simpler on paper.
What if the person also has anxiety depression or bipolar disorder
That changes the assessment. Alcohol withdrawal and psychiatric symptoms can look similar in the first days. Agitation, panic, insomnia, racing thoughts, and restlessness do not always come from one cause.
That overlap is one reason outpatient detox is not appropriate for everyone. If bipolar disorder, major depression, panic symptoms, trauma symptoms, or suicidal thinking may be involved, the detox plan needs closer clinical supervision and coordination with mental health care.
What should a family do right now
Start with immediate safety. If the person is confused, hallucinating, having a seizure, hard to wake, struggling to breathe, or becoming unresponsive, get emergency medical help now.
If they are uncomfortable but stable, gather the details a detox team will ask for: when they had their last drink, how much they usually drink, whether they have ever had seizures or delirium during withdrawal, what medications or substances are involved, and whether there are mental health concerns. That information helps a clinician decide whether a fixed-dose taper, symptom-triggered monitoring, or inpatient detox is the safer call.
Families also help by avoiding common mistakes:
- Do not wait for symptoms to “wear off.” Withdrawal can worsen after a brief calm period.
- Do not use a borrowed taper schedule. A plan that was tolerated by one person can be unsafe for another.
- Do not treat psychiatric symptoms as separate from detox. Panic, depression, confusion, and insomnia all affect the treatment plan.
- Do not assume home is the safest setting. The right setting depends on risk, monitoring, and how reliably the patient can be reassessed.
Early evaluation is safer than trying to catch up after withdrawal becomes severe.
If alcohol withdrawal has started, or the family is trying to prevent a crisis from escalating, Tru Dallas Detox & Recovery Center can provide a confidential assessment, insurance verification, and clear guidance on the safest next step.