Some readers arrive at this topic after months of second-guessing. They’ve taken gabapentin exactly as prescribed, or they started taking more than intended, and now they want off. What stops them is usually the same fear. What happens if the dose drops too fast, sleep disappears, anxiety spikes, pain returns, or something more serious happens in the middle of the night?
That fear isn’t irrational. Tapering off gabapentin can be straightforward for some people and unexpectedly difficult for others. The difference often comes down to dose, length of use, other substances, and whether depression, anxiety, bipolar disorder, alcohol use, or another co-occurring condition is already in the picture.
The safest message is also the simplest one. Don’t stop gabapentin abruptly without medical guidance. A structured taper gives the nervous system time to adjust, lets a clinician watch for warning signs, and creates room to slow down if symptoms become hard to manage. For many people in Dallas and the surrounding DFW area, that turns a frightening process into a manageable one.
Table of Contents
- The First Step Toward Freedom from Gabapentin
- Why a Gradual Taper Is Medically Necessary
- Recognizing Gabapentin Withdrawal Symptoms and Timeline
- Designing a Safe Tapering Plan with Your Doctor
- When Professional Detox in Dallas is The Safest Choice
- Begin Your Recovery Journey with Tru Dallas Detox
The First Step Toward Freedom from Gabapentin
A common pattern looks like this. Someone misses a refill, tries to stretch the remaining capsules, and suddenly feels far worse than expected. Another person decides it’s time to quit because the medication no longer feels helpful, only to realize that “just stopping” isn’t a safe plan.
That moment matters because it changes the question. The goal is no longer just getting off the medication. The goal is getting off safely, without creating a crisis that could have been prevented.
For some patients, online advice makes this sound easier than it is. Lists of sample schedules can be useful, but they often leave out the hardest cases. They don’t account for the person taking gabapentin along with other psychiatric medications. They don’t account for someone with alcohol use disorder, chronic insomnia, panic symptoms, or a past history of severe withdrawal from another substance.
What tends to work and what usually doesn't
A safer path usually includes a prescribing clinician, a written taper plan, symptom tracking, and a clear backup plan if the reduction feels too aggressive.
What usually goes badly is more predictable:
- Stopping cold turkey: This can trigger an abrupt rebound in symptoms and can become medically dangerous.
- Cutting too much at once: Large reductions may look efficient on paper but often fail in real life when the body pushes back.
- Ignoring mental health symptoms: Mood destabilization, agitation, and insomnia can become the reason a taper collapses.
- Trying to “tough it out” alone: A person may wait too long to seek help because they assume suffering means the taper is working.
Practical rule: A successful gabapentin taper isn’t the fastest one. It’s the one the patient can actually tolerate and finish.
In Dallas detox settings, the most productive starting point is an honest assessment of risk. If the use has been long-term, if other substances are involved, or if mental health symptoms already feel unstable, the taper needs more than willpower. It needs structure. That’s the first real step toward freedom from gabapentin.
Why a Gradual Taper Is Medically Necessary

A gradual taper protects the brain and body from abrupt change. Gabapentin affects how the nervous system regulates excitability, sleep, pain signaling, and anxiety. After regular use, especially over months or years, the body adjusts to having the medication on board. Removing it too quickly can trigger a destabilizing rebound.
That risk rises in the patients standard online advice usually overlooks. I am talking about people with panic disorder, bipolar symptoms, major depression, chronic insomnia, alcohol or benzodiazepine use, or a long history of daily gabapentin. In those cases, tapering is not just about getting off a medication. It is about preventing a manageable reduction from turning into a psychiatric or medical crisis.
Dependence develops through adaptation
Physical dependence can happen even when gabapentin was taken exactly as prescribed. That does not mean addiction. It means the nervous system adapted to repeated exposure and now needs time to readjust.
The FDA has also warned that gabapentinoids can create serious risks in some patients, particularly when combined with other central nervous system depressants or used in people with respiratory risk factors, which is one reason medication changes should be handled cautiously and under medical supervision, as described in this FDA safety communication on gabapentinoids.
A taper lowers that stress on the system by reducing the dose in stages. The exact schedule depends on the patient’s daily dose, reason for use, other medications, past withdrawal history, and mental health stability. There is no single template that fits everyone safely.
Why supervision changes the safety picture
The main problem is not discomfort alone. It is variability.
One patient may do well with an early reduction and then fall apart after several smaller cuts. Another may develop severe insomnia within days, which then worsens anxiety, mood symptoms, and cravings for other substances. Someone with co-occurring mental health conditions can look stable at baseline and still decompensate once sleep and nervous system regulation start to slip.
That is where home taper attempts often fail. The plan may look reasonable on paper, but no one is adjusting it in real time.
Medical oversight allows for dose holds, smaller step-downs, medication review, and monitoring for warning signs that should not be pushed through. Patients and families also need to know the difference between expected discomfort and danger signs that call for prompt help. Our guide on what detox symptoms are normal and when to get medical help can help frame that decision.
A medically supervised taper becomes more important in situations like these:
| Situation | Why it changes the taper |
|---|---|
| Long-term gabapentin use | The nervous system has had more time to adapt, so reductions may need to be slower |
| Higher daily doses | Larger dose cuts can produce sharper rebound symptoms |
| Co-occurring psychiatric conditions | Anxiety, insomnia, mood instability, and agitation can escalate quickly |
| Use of alcohol, benzodiazepines, or other sedating drugs | Overlapping withdrawal or sedation risks make self-management less reliable |
| Prior failed taper attempts | Earlier setbacks often show that the original pace was too aggressive |
For higher-risk patients in Dallas, the trade-off is simple. A faster taper may sound efficient, but it often increases the chance of destabilization, relapse, or an emergency evaluation. A slower, medically supervised taper usually gives the patient the best chance to finish safely.
Recognizing Gabapentin Withdrawal Symptoms and Timeline
A patient may stop gabapentin expecting a few restless nights, then find that by the second day they cannot sleep, their anxiety is spiking, and the pain or mood symptoms that led to treatment in the first place feel worse. That situation becomes more complicated when the person also has panic disorder, depression, trauma symptoms, or a history of using alcohol or sedatives. Standard online advice often treats withdrawal like a simple countdown. In higher-risk patients, it is a moving clinical picture that needs close attention.
What withdrawal can feel like
Gabapentin withdrawal can affect the body, mood, sleep, and thinking at the same time. Patients often describe a cluster of symptoms rather than one clear complaint.
Common symptoms include:
- Sleep disruption: Trouble falling asleep, repeated waking, vivid dreams, or waking in panic
- Anxiety and agitation: Feeling keyed up, restless, irritable, or unable to settle
- Stomach symptoms: Nausea, reduced appetite, abdominal upset
- Rebound symptoms: Nerve pain, burning sensations, headaches, or emotional symptoms that return after the dose drops
- Physical distress: Sweating, tremor, fatigue, chills, and a flu-like sense of feeling unwell
- Mood changes: Irritability, low mood, emotional swings, or a sense of feeling unlike oneself
- Cognitive strain: Poor concentration, mental fog, or feeling overwhelmed by ordinary tasks
For patients with co-occurring mental health conditions, the hardest part is often not the symptom itself. It is the uncertainty about what the symptom means. A person with generalized anxiety may assume rising panic is just their baseline condition coming back. A person with depression may see insomnia and emotional volatility as personal failure rather than a medication effect. That confusion leads people to restart the drug abruptly, give up on treatment, or delay getting help when the taper clearly needs adjustment.
Symptom intensity matters. It gives the clinician useful information about whether the taper is tolerable or too aggressive.
Some discomfort can happen during a taper. Escalating anxiety, severe insomnia, marked agitation, or concerning physical symptoms should trigger reassessment.
Families should also know what falls inside the expected range and what deserves urgent medical attention. Our guide to detox symptoms, what is normal, and when to get medical help can help with that distinction.
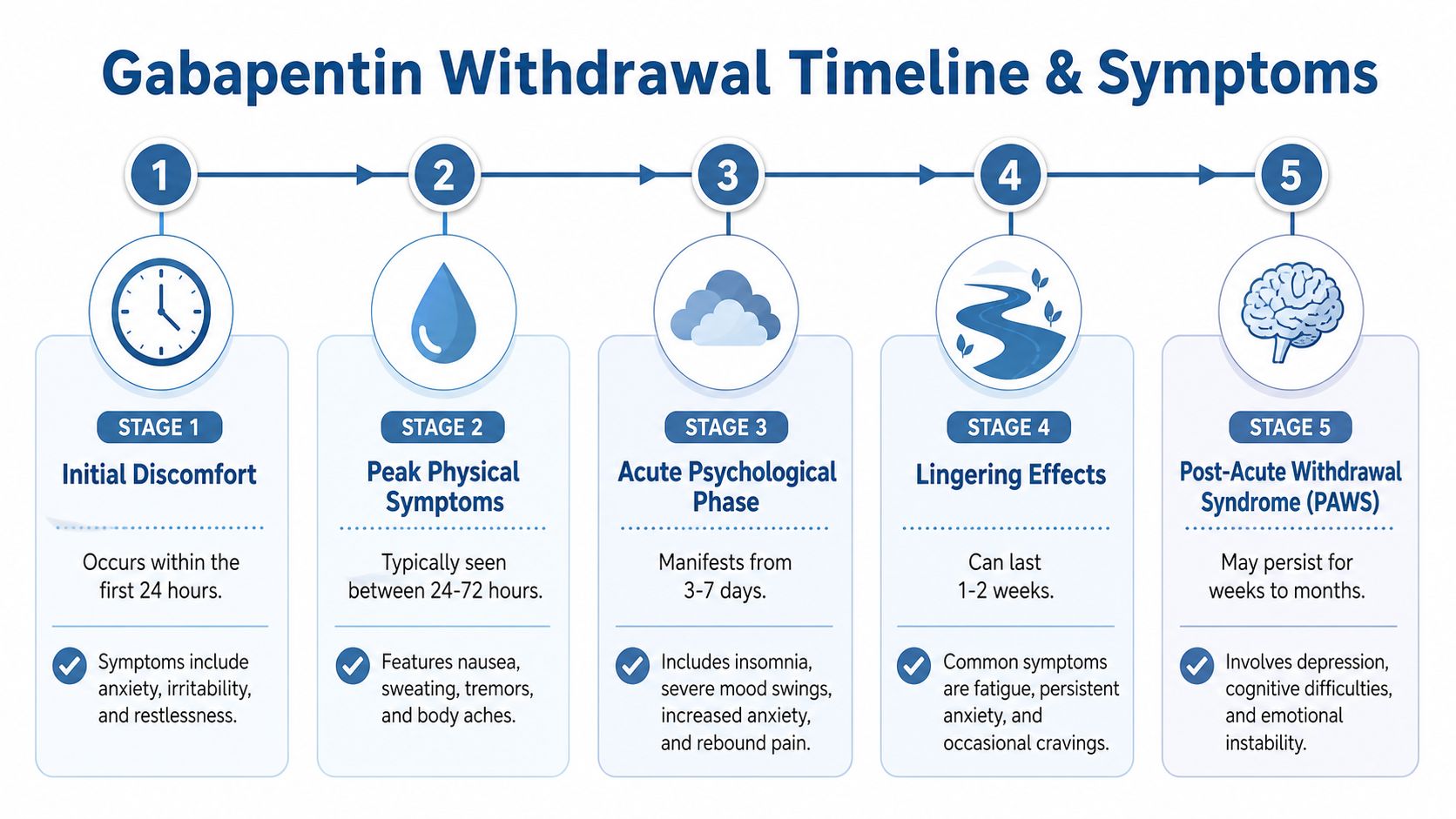
A practical timeline to expect
Withdrawal symptoms often begin within the first couple of days after a major dose reduction or abrupt stop. Early symptoms tend to involve sleep disruption, restlessness, sweating, and anxiety. For some patients, that first phase is manageable. For others, especially those with long-term use or psychiatric instability, it can escalate fast.
The middle of the withdrawal period is usually the hardest. This is when physical discomfort, rebound pain, agitation, and mood instability may feel most disruptive. Patients with bipolar symptoms, severe anxiety, or trauma-related hyperarousal often struggle more in this window because withdrawal can amplify the same systems that are already vulnerable.
Acute symptoms usually improve over days to weeks, but recovery is not always linear. Sleep may remain poor after the worst physical symptoms ease. Mood and stress tolerance can also lag behind. In practice, that longer tail is one reason self-directed tapers fail. The patient may be technically off gabapentin but still too destabilized to function safely at home, at work, or in early recovery from other substances.
There is also a safety issue that should be stated plainly. Abrupt discontinuation can be dangerous, and the risk rises in patients on high doses, with seizure history, with polysubstance use, or with co-occurring psychiatric illness. Those are the Dallas patients I worry about most, because they are the ones least likely to do well with generic online taper schedules and most likely to benefit from medical detox or close outpatient supervision.
A simple way to frame the timeline is:
- Early phase: Sleep changes, anxiety, restlessness, sweating, and physical unease begin after a dose reduction or sudden stop.
- Peak phase: Distress is often strongest here. Rebound pain, agitation, nausea, tremor, and mood symptoms can become hard to manage.
- Stabilization phase: Acute symptoms start to settle, but sleep, energy, and emotional steadiness may recover more slowly.
- Lingering phase: Some patients continue to have insomnia, anxious distress, or mood fragility after the acute withdrawal period has passed.
That last phase is where standard advice often falls short. Patients with depression, anxiety disorders, PTSD, or long-term gabapentin exposure may need more than a taper calendar. They may need medication review, symptom monitoring, sleep support, and a higher level of care if functioning starts to unravel.
Designing a Safe Tapering Plan with Your Doctor
A taper plan should never be copied blindly from the internet. It should be built around the patient in front of the clinician. Dose matters, but it isn’t the only variable. Duration of use, kidney function, sleep quality, substance use history, and psychiatric stability all shape how a taper should proceed.
What a conservative taper usually looks like
A common medical framework is a 10% to 25% reduction every 1 to 2 weeks. One published example describes a patient on 1800 mg/day stepping down to 1500 mg for two weeks, then 1200 mg, with smaller reductions once the dose falls below 600 mg. That same guidance notes that supervised tapers achieve over 90% success without major complications when the plan stays flexible and symptom-informed, as described in this tapering overview.
The reason lower doses often require smaller cuts is simple. The final stretch can be the most sensitive part of the taper. A reduction that felt tolerable earlier may feel much harder later.
What should be reviewed before the first dose reduction
Before a doctor changes the dose, several questions should be answered clearly:
- Why is gabapentin being stopped now: Side effects, misuse, limited benefit, interaction concerns, or a broader addiction treatment plan all call for slightly different approaches.
- What else is the patient taking: Other sedating medications, stimulants, alcohol, and illicit substances can complicate the picture quickly.
- What happened during past taper attempts: Prior insomnia, panic, rebound pain, or seizures should influence the pace.
- What support is available at home: A careful plan can still fail if the patient is isolated or unable to report worsening symptoms.
A useful taper conversation also includes what happens if symptoms flare. Does the clinician hold the dose steady? Reduce more slowly? Switch the timing of doses? Bring the patient in for closer monitoring? The answers should be clear before the first cut is made.
| Taper planning question | Why it matters |
|---|---|
| How long has the patient been taking gabapentin? | Longer use can call for more caution |
| Is there co-occurring anxiety, depression, or bipolar disorder? | Mental health symptoms may destabilize during tapering |
| Has the patient misused alcohol or other drugs? | Withdrawal overlap may increase risk |
| What does the patient do if symptoms become severe? | Clear instructions prevent panic and dangerous self-adjustment |
Another important point is treatment setting. Some patients can taper as outpatients with close follow-up. Others need a higher level of support, especially if gabapentin misuse is part of a broader substance use disorder. For readers comparing options, this explanation of medication-assisted treatment helps clarify how structured medical support fits into a larger recovery plan.
The best taper plan is specific enough to guide care and flexible enough to change when the patient’s symptoms change.
When Professional Detox in Dallas is The Safest Choice
Some situations move beyond “talk to a doctor” and into “this needs a monitored setting.” That threshold arrives sooner than many families expect, especially when gabapentin use overlaps with alcohol, benzodiazepines, stimulants, or unstable mental health symptoms.

Red flags that make home tapering risky
A home taper may be too risky when any of the following are present:
- Long-term use with failed prior tapers: Repeated attempts that end in severe symptoms usually mean the taper needs more structure.
- Co-use of alcohol or sedatives: Withdrawal syndromes can overlap and become harder to evaluate safely.
- Psychiatric instability: If the person already has severe anxiety, depression, panic, or mood swings, dose reductions can intensify the problem.
- Misuse patterns: Taking more than prescribed, running out early, or using gabapentin to manage the effects of other substances raises the risk profile.
- Unreliable support at home: Even a well-designed outpatient taper depends on communication, monitoring, and follow-through.
In those cases, a Dallas detox center can provide something a home setting can’t. Continuous observation, rapid medication adjustments, and coordinated psychiatric support.
Why dual diagnosis changes the plan
The biggest gap in standard online advice is how little it says about co-occurring mental health conditions. A taper isn’t happening in a vacuum. If the patient has depression, anxiety, bipolar disorder, trauma symptoms, or another substance use disorder, each dose reduction can affect more than withdrawal alone.
That’s one reason severe cases can become surprisingly long. A published case report described a patient with alcohol use disorder who required an 18-month gabapentin taper, with reductions eventually as small as 5 mg at a time to control withdrawal symptoms, as detailed in this case summary of complex gabapentin tapering.
That case shouldn’t be read as typical for everyone. It should be read as a warning against oversimplification.
When alcohol use, psychiatric symptoms, and long-term gabapentin dependence overlap, the taper often needs more time and more clinical support than generic advice suggests.
For many higher-risk patients in Dallas, Frisco, Plano, Irving, Euless, and across DFW, professional detox is the safer choice because it allows one team to monitor the whole picture. Readers considering that level of care can review what medically supervised detox in Dallas involves and compare it to the risks of trying to manage a complex taper alone.
Begin Your Recovery Journey with Tru Dallas Detox
The hardest part for many families isn’t deciding that help is needed. It’s figuring out what happens after that decision. They want to know who monitors symptoms, what happens if the taper takes longer than expected, and whether treatment can address both substance use and mental health at the same time.

A strong program should handle more than the acute withdrawal window. Some patients continue to struggle with sleep, anxiety, mood changes, or concentration problems after the initial detox phase. That matters because insurance timelines don’t always match clinical timelines. As noted in this discussion of post-acute withdrawal planning and coverage gaps, a significant care gap can emerge when inpatient coverage ends before symptoms fully stabilize, making step-down planning and outpatient support essential.
What support should look like after detox
For someone tapering off gabapentin, good care usually includes several layers at once:
- Medical monitoring during dose changes: The team should track symptom patterns and respond quickly if the taper needs to slow.
- Psychiatric support: If mood, anxiety, or sleep destabilizes, those symptoms need active treatment, not dismissal.
- Transition planning: Patients need a realistic bridge from detox to outpatient care, not a vague instruction to “follow up somewhere.”
- Family guidance: Loved ones often need help understanding what’s expected, what’s concerning, and how to support recovery without increasing stress.
Some patients also benefit from flexible follow-up models after detox. For readers exploring broader recovery options, Integrative Psychiatry of America's insights offer a useful perspective on how continued treatment access can support stability when in-person care isn’t needed at the same intensity every day.
What families in Dallas should do next
If a loved one is trying to stop gabapentin and the process already feels chaotic, that’s enough reason to pause and get help. Waiting for the situation to become dramatic usually makes treatment harder, not easier.
Families in Dallas often ask the same practical questions first:
Can insurance be checked before admission?
It should be. Verifying PPO benefits early helps families make decisions without guessing.What if the taper needs more time than expected?
The program should have a step-down plan in place before discharge.Can treatment address mental health too?
It needs to. Dual diagnosis care isn’t optional when psychiatric symptoms are part of the risk.What if the patient is ashamed or afraid to call?
That’s common. A good admissions process meets people where they are and starts with clarity, not pressure.
Recovery from gabapentin dependence can start in a subtle way. Sometimes it begins with one honest phone call, one review of medications, or one decision not to attempt another solo taper. For many patients in the Dallas area, that first safe step changes everything.
If you or someone you love is struggling with tapering off gabapentin, Tru Dallas Detox & Recovery Center can help with confidential guidance, PPO insurance verification, medically supervised detox, and dual diagnosis support for complex cases across Dallas-Fort Worth. Reach out today to discuss the safest next step.