
Some people in Dallas are living through the same pattern right now. A few nights of very little sleep turn into racing thoughts, bigger risks, more drinking, or drug use that feels easier to justify in the moment. Then the crash comes. Work suffers, relationships strain, medications get skipped, and everyone in the family starts arguing about what the actual problem is.
That pattern often isn't “just addiction” or “just mood swings.” It can be substance abuse bipolar disorder, a co-occurring condition in which bipolar disorder and a substance use disorder feed each other. For many families across Dallas-Fort Worth, the hardest part isn’t lack of effort. It’s that the symptoms overlap, the crises escalate fast, and single-focus treatment often misses the full picture.
When bipolar disorder and substance use are treated separately, people often keep circling back into the same emergencies. That’s one reason dual diagnosis care matters so much. The overlap is common, serious, and treatable. The lifetime prevalence of substance use disorders in patients with bipolar disorder is at least 40%, with some studies reporting rates as high as 61%, according to research on bipolar disorder and substance use comorbidity.
Table of Contents
- Understanding the Connection Between Bipolar Disorder and Addiction
- The Vicious Cycle of Self-Medication and Impulsivity
- Recognizing the Overlapping Signs and Symptoms
- Clinical Risks and Complications of Untreated Dual Diagnosis
- How to Get an Accurate Dual Diagnosis Assessment in Dallas
- Evidence-Based Integrated Treatment at Tru Dallas Detox
- Your Path to Recovery Begins Today Your Next Steps
Understanding the Connection Between Bipolar Disorder and Addiction
Bipolar disorder changes energy, sleep, judgment, and emotional intensity. Addiction changes reward, behavior, and self-control. When they appear together, the result is more than the sum of two diagnoses. Each condition makes the other harder to recognize and harder to treat.
Clinicians call this a dual diagnosis or co-occurring disorder. For the person living through it, it can feel less clinical and more chaotic. One week may look like depression with drinking to shut off emotional pain. Another may look like agitation, overspending, drug use, and a complete loss of perspective.
Why this combination is so common
Substances can seem useful at first. Alcohol may feel like a way to slow down. Sedatives may look like sleep help. Stimulants may seem like a shortcut through depression or a way to ride the energy of a manic state.
That short-term relief is misleading. The nervous system doesn’t stay neutral. Mood becomes less predictable, treatment becomes less consistent, and crises become more frequent.
- Mood symptoms get blurred: Families often can’t tell whether they’re seeing mania, withdrawal, intoxication, or depression.
- Treatment gets fragmented: One provider may focus on sobriety while another focuses on mood, and neither gets the full picture.
- Shame grows fast: People often blame themselves for “failing” when the underlying issue is untreated dual diagnosis.
A broader look at mental health and substance abuse can help families understand why these conditions so often overlap.
Clinical reality: People with co-occurring bipolar disorder and addiction usually need one coordinated plan, not two separate conversations happening in parallel.
Why hope is realistic
This condition is serious, but it’s treatable. Accurate assessment, safe detox when needed, mood stabilization, and therapy that addresses both illnesses at the same time can change the trajectory. For people in Dallas, Plano, Irving, Euless, Arlington, and the wider DFW area, the key is getting care from a program that understands both the psychiatric side and the addiction side from day one.
The Vicious Cycle of Self-Medication and Impulsivity

Substance abuse in bipolar disorder often stems from two primary drivers. The first is self-medication. The second is impulsivity during heightened mood states. Both feel understandable in the moment. Both make the illness harder to control.
During depression, alcohol or pills may seem like a way to numb dread, slow intrusive thoughts, or get through a night that feels unbearable. During mania or hypomania, the pattern shifts. Judgment loosens, confidence rises, sleep drops, and the brain stops weighing consequences the way it normally would.
When substances feel like symptom relief
People don’t usually start from a place of wanting a dual diagnosis. They start from distress. They want sleep. They want quiet. They want relief from despair, agitation, irritability, or inner pressure.
The problem is that substances change the course of bipolar symptoms rather than fixing them.
| Phase | What the person may want | What substance use often does |
|---|---|---|
| Depression | Numb sadness, sleep, emotional escape | Deepens instability, disrupts treatment, adds dependence |
| Mania or hypomania | More energy, less inhibition, prolonged high | Increases risk-taking, worsens judgment, fuels escalation |
| Mixed symptoms | Relief from agitation and despair at the same time | Creates a highly unstable and dangerous pattern |
A useful way to think about it is a pendulum. Bipolar disorder already creates swings. Substance use pushes the pendulum wider, faster, and harder to stop.
Why mania raises the stakes
The association between mania and addiction risk is particularly strong. During manic episodes, individuals with bipolar disorder are 14 times more likely to have a drug abuse disorder and 6 times more likely to have an alcohol abuse disorder, according to clinical reporting on bipolar disorder and substance abuse.
That matters in real life because manic vulnerability rarely shows up as one simple symptom. It may show up as:
- Decreased sleep: Staying awake without feeling tired, then using substances to stay up longer or come down.
- Grandiosity: Believing consequences don’t apply, or assuming use is under control despite obvious fallout.
- Fast decisions: Spending, driving, sexual risk, and drug seeking all become easier to justify.
- Irritability: Arguments escalate, family members pull back, and the person becomes less reachable.
A relapse plan for bipolar disorder that ignores manic warning signs usually isn't strong enough.
What doesn’t work
Treating every episode as a willpower problem usually fails. So does trying to stabilize mood while substance use continues unchecked. In Dallas addiction treatment settings, the most effective approach is usually the one that addresses cravings, sleep disruption, medication adherence, and bipolar symptom patterns together instead of in separate silos.
Recognizing the Overlapping Signs and Symptoms

The hardest part for many families isn’t seeing that something is wrong. It’s figuring out what they’re seeing. Bipolar disorder can look like intoxication. Substance use can look like mania, anxiety, or depression. That confusion is one reason people spend years in the wrong kind of treatment.
Research has shown that substance abuse often delays or obscures a correct bipolar diagnosis because drug effects such as euphoria or paranoia can mimic mood episodes, as discussed in research on diagnostic masking in bipolar disorder and substance use.
Signs that point more toward bipolar disorder
These symptoms matter most when they show up as recurring mood episodes rather than isolated bad days.
- Manic features: Reduced need for sleep, racing thoughts, inflated confidence, intense goal-directed activity, agitation, and risky behavior.
- Depressive features: Hopelessness, low energy, slowed thinking, loss of interest, guilt, isolation, or thoughts of self-harm.
- Cycling pattern: Shifts between manic and depressed states, sometimes with stretches of relative stability in between.
Signs that point more toward a substance use disorder
These signs usually center on loss of control and continued use despite harm.
- Compulsive use: Repeated use even after job problems, relationship damage, health scares, or legal trouble.
- Tolerance and withdrawal: Needing more of a substance, or feeling sick, shaky, anxious, or distressed when stopping.
- Preoccupation: Spending large amounts of time getting, using, recovering from, or hiding substances.
Signs that overlap and confuse the picture
Many families find themselves stuck at this point.
- Sleep disruption: Staying up all night may be mania, withdrawal, intoxication, or medication side effects.
- Irritability: This can show up in depression, mania, stimulant use, alcohol misuse, or withdrawal.
- Poor judgment: Overspending, lying, impulsive sex, or aggression can stem from either condition.
- Paranoia or agitation: These can appear in manic states and with several substances.
- Inconsistent medication use: A person may stop psychiatric medication during mood elevation, during active use, or both.
Assessment clue: Clinicians need to ask what symptoms happen during active use, what symptoms happen during abstinence, and what pattern has repeated over time.
Sleep often becomes a major point of confusion. Families may focus on insomnia as the whole problem when it’s only one piece of a larger mood picture. For readers trying to understand practical strategies for coping with medication-induced sleeplessness, that issue can be relevant, but it still shouldn’t replace a full dual diagnosis evaluation.
Clinical Risks and Complications of Untreated Dual Diagnosis
Untreated dual diagnosis tends to become more disruptive over time. The person may keep moving between brief periods of control and severe destabilization. Loved ones often describe it as living in crisis management mode, always waiting for the next call, the next binge, the next disappearance, or the next argument that turns frightening.
This isn’t merely a matter of symptoms lasting longer. The course of illness often becomes more severe. Patients with both bipolar disorder and a substance use disorder experience significantly more psychiatric hospitalizations and are more likely to have a rapid-cycling pattern, according to findings on substance abuse in bipolar I disorder.
What gets worse when treatment is delayed
The damage usually shows up across multiple parts of life at once.
- Mood stability erodes: Episodes become harder to predict and harder to bring under control.
- Hospital care becomes more likely: Emergencies rise when mood symptoms and substance use amplify each other.
- Medication response gets harder to judge: It becomes difficult to tell whether a medication isn’t working or whether substances are overriding the benefit.
- Relationships fracture: Partners, parents, and children often swing between rescuing, arguing, and withdrawing.
- Work and finances suffer: Missed shifts, impulsive decisions, and inconsistent follow-through can build into major losses.
Why waiting is risky
People sometimes hope that sobriety alone will solve everything, or that psychiatric medication alone will make the addiction stop. That split approach often falls apart because each condition keeps reactivating the other.
A person may stop using briefly, then swing into mania and relapse. Another may restart psychiatric medication, but continue drinking heavily and never reach stable mood control. Families often read those setbacks as resistance. Clinically, they usually reflect untreated interaction between both disorders.
Untreated co-occurring bipolar disorder rarely stays contained. It tends to spread into safety, housing, relationships, employment, and physical health.
In Dallas and surrounding communities, the practical message is simple. If repeated relapses, erratic mood changes, medication inconsistency, and escalating consequences are all present, it’s time to seek a dual diagnosis level of care rather than another partial solution.
How to Get an Accurate Dual Diagnosis Assessment in Dallas
A Dallas family often reaches this point after a confusing stretch. A loved one has periods of high energy, little sleep, reckless decisions, or deep depression, while alcohol or drug use keeps changing the picture. One visit says addiction. Another says bipolar disorder. Neither answer fully explains what is happening.
An accurate dual diagnosis assessment separates overlapping symptoms instead of forcing a quick label. Clinicians need to map out what happened first, what shows up during active use, what continues during abstinence, and how sleep, stress, withdrawal, and prior medications affect the pattern. That level of detail helps prevent a common problem in co-occurring care. People get treated for the loudest symptom in the room while the underlying interaction between bipolar disorder and substance use goes unaddressed.
What a thorough assessment should include
A strong evaluation pulls information from several parts of the person’s history and current condition.
- Mood episode history: Clear descriptions of depressive, manic, hypomanic, or mixed symptoms, including duration, severity, and whether they appeared outside intoxication or withdrawal.
- Substance use timeline: Which substances are involved, when use escalated, what happens during withdrawal, and whether the person uses to slow racing thoughts, lift depression, sleep, or numb agitation.
- Medication history: Prior psychiatric medications, side effects, missed doses, activation, sedation, and whether any medication seemed to worsen impulsivity, insomnia, or mood instability.
- Family psychiatric history: Bipolar disorder, addiction, suicide attempts, psychosis, and other major mental health conditions in close relatives.
- Daily functioning: Changes in judgment, parenting, work performance, finances, relationships, driving safety, and legal stress.
- Immediate risk: Suicidal thinking, self-harm, psychosis, aggression, inability to sleep, overdose history, or medical instability.
Some readers already understand the value of broad health screening from resources such as Lola's full body check. The same principle applies here. A narrow intake misses the pattern that determines safe treatment.
What people in DFW should look for
In practice, the right assessment feels careful and specific. It includes collateral information from family when available, a review of prior records, screening for withdrawal risk, and direct questions about sleep, spending, sexual impulsivity, agitation, and periods of depression that may have been hidden under substance use. It also leaves room for diagnostic clarification over time, because some cases become clearer only after detox and early stabilization.
Dallas residents should also ask a practical question. Can the program assess and treat both conditions in the same setting, or will psychiatric care and addiction care stay split between different providers? Split care often leads to mixed messages, duplicated medications, and missed warning signs.
For local families trying to understand what appropriate next-step care should include, bipolar disorder treatments near me is a useful starting point.
One local option is Tru Dallas Detox & Recovery Center, which provides medically supervised detox, dual diagnosis treatment, inpatient and outpatient rehab, medication-assisted treatment, and aftercare planning for people in the Dallas-Fort Worth area. For substance abuse bipolar disorder, that coordinated structure matters because diagnostic review, withdrawal management, and treatment planning can happen together instead of in isolation.
Evidence-Based Integrated Treatment at Tru Dallas Detox
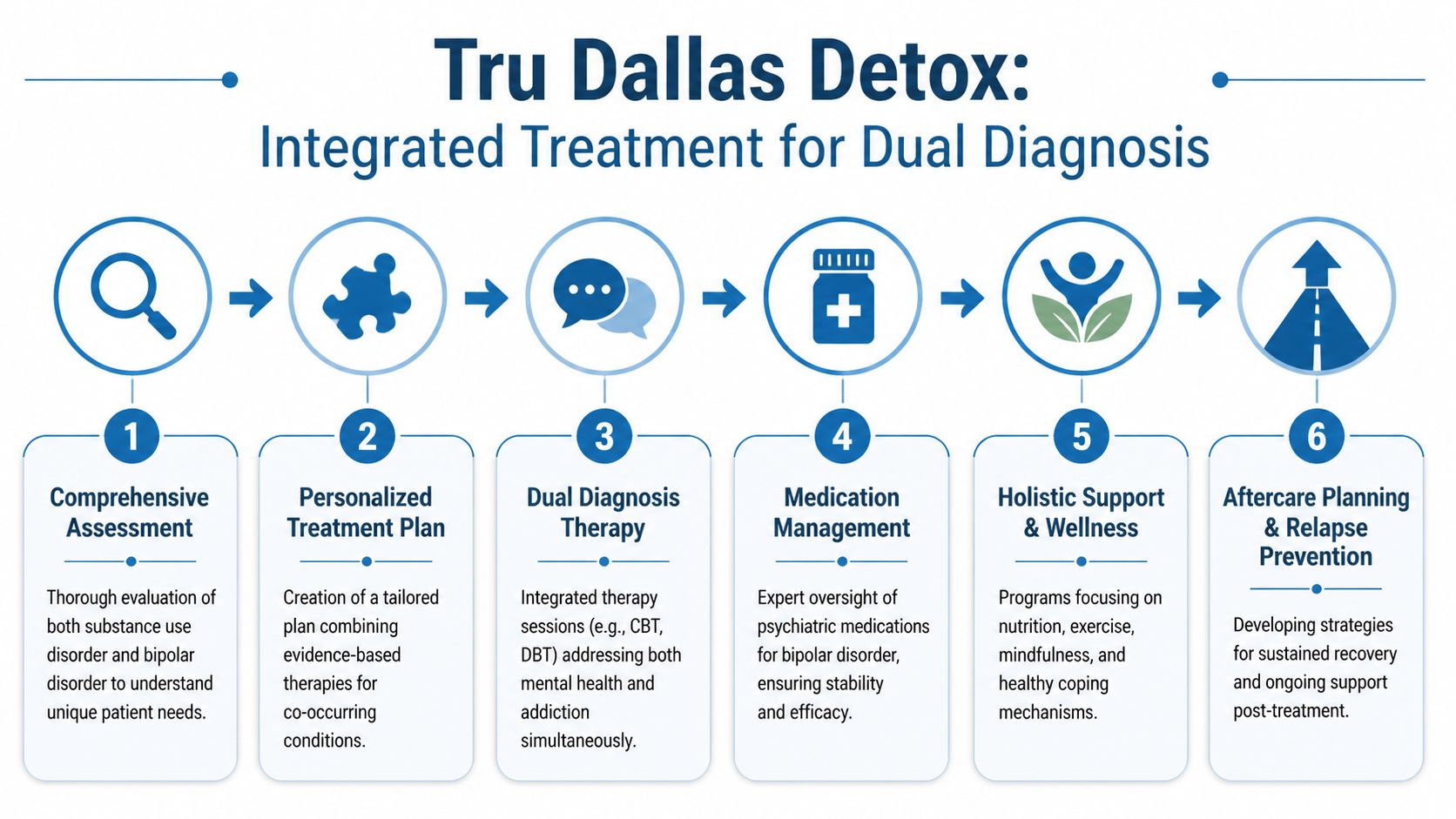
People with bipolar disorder and addiction usually don’t need a single intervention. They need a sequence. The order matters, the pacing matters, and the communication between providers matters.
When treatment works, it usually does four things well. It stabilizes the body, clarifies the diagnosis, treats both disorders at the same time, and keeps support in place after the first crisis passes.
Medical stabilization comes first
Detox is often the first practical step when alcohol, opioids, sedatives, or other drugs are actively involved. For a person with bipolar disorder, withdrawal can intensify insomnia, agitation, fear, and emotional volatility. That’s why medical supervision matters. It reduces the chance that withdrawal symptoms will be mistaken for purely psychiatric deterioration, or that psychiatric symptoms will be ignored as “just detox.”
A safe detox setting also gives clinicians a clearer window into what mood symptoms remain once acute substance effects begin to settle.
Rehab has to treat both conditions together
Inpatient rehab can help when the person is unstable, repeatedly relapsing, or unsafe at home. Outpatient care can work well when there’s enough structure, transportation, and family support to maintain continuity. The key isn’t choosing the most intensive setting by default. It’s matching the setting to the current level of risk.
What usually works best in either level of care:
- One treatment plan: Bipolar symptoms and substance use are addressed together instead of by separate teams with separate goals.
- Clear routines: Regular sleep, medication timing, meals, therapy, and check-ins help reduce chaos.
- Relapse prevention tied to mood warning signs: Plans should account for both cravings and early manic or depressive shifts.
Medication and therapy work better when coordinated
Medication can play an important role in reducing instability, but only when clinicians track it alongside substance use, sleep, side effects, and adherence. For some patients, medication-assisted treatment is also part of the plan. Readers exploring what medication-assisted treatment involves often find that it helps clarify how addiction medications fit into a broader recovery plan rather than replacing therapy or psychiatric care.
Therapy also has to be practical. Patients need help identifying what precedes use, what precedes mood shifts, and what daily structure protects recovery.
A coordinated therapy plan often includes:
- Cognitive work that challenges all-or-nothing thinking, grandiosity, hopelessness, and relapse justifications.
- Behavioral structure that protects sleep, routines, medication consistency, and appointment follow-through.
- Family involvement so loved ones know the difference between support, enabling, and emergency response.
What works: treatment that links sleep loss, mood elevation, craving, and relapse in one clinical plan.
A more integrated psychotherapy model matters because single-focus care often misses the interaction effect between disorders. Some evidence-based integrated approaches have shown meaningful results. Integrated Bipolar-C SUD Therapy has been shown to cut hospital readmissions by 45%, and quetiapine has been reported to reduce substance cravings by 40% in dual diagnosis patients, according to discussion of integrated bipolar and substance use treatment.
Aftercare is where stability gets protected
The first good week isn’t the goal. Lasting recovery is. That means discharge planning should be built around real triggers, not generic advice.
Aftercare usually needs to cover:
- Medication follow-up: Ongoing psychiatric monitoring, especially after detox or medication changes.
- Therapy continuity: The same relapse themes need to be addressed after discharge, not restarted from zero.
- Living environment: Some people need sober housing or a more protected setting before returning home.
- Family expectations: Everyone needs a plan for warning signs, communication, transportation, and crisis steps.
For Dallas detox center and addiction treatment in Dallas searches, the strongest clinical filter is simple. Look for a program that treats bipolar disorder and substance use as one intertwined illness pattern, not two separate administrative boxes.
Your Path to Recovery Begins Today Your Next Steps
The next move doesn’t have to be dramatic. It has to be clear. If someone is showing signs of substance abuse bipolar disorder, the most useful step is to stop arguing about labels and start arranging a proper evaluation and safe treatment entry.

Families often wait because they’re hoping for a calmer week, a sincere promise, or one more sign that the person is ready. In reality, readiness often grows after structure begins, not before. Co-occurring disorders are also seen more often in certain profiles, including younger individuals and with a male predominance, according to hospital and demographic findings on bipolar disorder with substance use. That kind of pattern matters because treatment planning often has to account for family conflict, immaturity in coping skills, and unstable daily routines.
What families can do right now
A helpful response is calm, direct, and practical.
- Focus on safety first: If there’s severe agitation, suicidal thinking, inability to sleep for an extended period, psychosis, or heavy intoxication, seek immediate professional help.
- Use concrete language: Point to missed work, no sleep, unsafe driving, medication inconsistency, or escalating use. Avoid debates about character.
- Set one next step: A call, an assessment, insurance verification, or transport plan is more useful than a long argument.
- Protect the home: Remove obvious substances when possible, reduce conflict, and avoid late-night confrontations during intoxication or mania.
What to ask when calling for help in Dallas
The right questions save time and reduce confusion.
- Ask about dual diagnosis capability: Can the program assess bipolar disorder and addiction together?
- Ask about detox access: If withdrawal is likely, is medical monitoring available?
- Ask about medication coordination: How are psychiatric medications handled alongside addiction treatment?
- Ask about aftercare: What happens after detox or rehab ends?
- Ask about insurance: Can the team verify PPO coverage before admission?
Sleep support is often part of stabilization, but it should never become the whole treatment plan. Families looking at conservative sleep strategies may appreciate guidance on SleepHabits natural insomnia relief, yet ongoing insomnia in the context of mood instability and substance use still calls for professional dual diagnosis care.
Recovery starts when the problem is named accurately and treated completely. For many people in Dallas, Fort Worth, Irving, Grapevine, Euless, and surrounding areas, that means getting help before the next manic shift, relapse, overdose risk, or psychiatric emergency takes over again.
If substance abuse and bipolar symptoms are colliding in your life or in someone you love, Tru Dallas Detox & Recovery Center can help you take the next step. Reach out for a confidential conversation, ask about PPO insurance verification, and get clear guidance on detox, dual diagnosis assessment, and treatment options in the Dallas-Fort Worth area.