
A lot of people reach this point without much fanfare. The crisis phase is over. They’re no longer waking up sick, chasing pills, or wondering how they’ll get through the day. They’ve been taking Suboxone for a year or longer, life has stabilized, and a new question starts to matter: What happens if this continues long term?
That’s a reasonable question. It doesn’t mean treatment has failed. It usually means recovery has progressed enough for someone to think beyond immediate survival and focus on long-term health, mood, energy, sleep, teeth, hormones, and quality of life.
Suboxone remains one of the most important medications used in opioid recovery. It can reduce cravings, lower the danger of relapse, and give people enough stability to rebuild work, family, and mental health. At the same time, suboxone side effects long term are real. Some are mild and manageable. Some deserve medical follow-up. A few are often missed because people assume they’re “just stress” or “just getting older.”
Table of Contents
- Starting the Conversation About Long-Term Suboxone Use
- Why Suboxone is a Long-Term Treatment Strategy
- Navigating Long-Term Physical Side Effects
- Understanding the Psychological and Emotional Impact
- Suboxone's Benefits vs Risks of Relapse
- How to Manage Side Effects and Improve Your Quality of Life
- Find Your Path Forward at Tru Dallas Detox & Recovery Center
Starting the Conversation About Long-Term Suboxone Use
For many people in Dallas and Fort Worth, the hardest part of opioid recovery isn’t starting treatment. It’s trusting what comes next. Once the chaos settles, concerns shift from withdrawal and cravings to questions about mood, hormones, sleep, dental health, and whether staying on medication still makes sense.
That concern deserves a direct answer. Suboxone can be a life-saving medication, and it can also create long-term issues that need monitoring. Both can be true at the same time. Oversimplified advice usually causes harm. Telling patients to stay on it forever without follow-up is careless. Telling them to stop quickly because “you shouldn’t need it anymore” can be dangerous.
Key takeaways: Long-term Suboxone use should be approached like any serious medical treatment. It works best when a patient’s physical health, mental health, and recovery goals are reviewed regularly, not assumed.
Some side effects show up clearly. Dry mouth, constipation, fatigue, and disrupted sleep get attention because they’re easy to name. Others develop more subtly. A patient may notice less interest in sex, less emotional range, more dental sensitivity, lower motivation, or a sense of feeling “flat” without realizing these changes could be related to long-term medication use.
Families in the Dallas area often miss this too. They may see a loved one who’s no longer using illicit opioids and assume everything is solved. Recovery is better than it was, but that doesn’t mean the work is finished. Long-term medication-assisted treatment still requires monitoring, especially when treatment extends well beyond the first year.
A balanced approach matters. The right question usually isn’t “Is Suboxone good or bad?” It’s “Is this treatment still helping more than it’s hurting, and is the current plan being managed well?” That’s the discussion patients deserve from any Dallas detox center or addiction treatment program.
Why Suboxone is a Long-Term Treatment Strategy
Suboxone isn’t only used to get someone through detox. For many patients, it becomes part of a longer recovery plan because opioid use disorder behaves like a chronic medical condition. Symptoms improve, then stress, grief, pain, isolation, or exposure to old triggers can bring risk back quickly.

How Suboxone works in plain language
Buprenorphine, the active ingredient in Suboxone, acts like a key that fits the opioid receptor but only turns part of the way. That partial activation matters. It can reduce withdrawal and cravings without creating the same level of intoxication people chase with heroin, fentanyl, or prescription opioids.
That’s why many physicians use it as a stabilizing medication instead of a short bridge only. Patients who want a simple breakdown of the medication itself can review how Suboxone works for addiction in plain language before deciding what questions to bring to their provider.
Suboxone also includes naloxone to discourage misuse. In treatment, the goal isn’t to sedate someone through life. The goal is to create enough steadiness that therapy, employment, parenting, sleep, and daily structure become possible again.
Dependence is not the same as addiction
Stigma causes confusion regarding these terms. Physical dependence means the body adapts to a medication and would likely react if it were stopped suddenly. That can happen with many legitimate prescriptions. Addiction involves compulsive use despite harm, loss of control, craving-driven behavior, and continued use even when life is unraveling.
Those are not the same thing.
A patient can be physically dependent on Suboxone and still be recovering well. A patient can also need dose adjustments, side-effect management, or a slower plan than expected. None of that means they’re “doing recovery wrong.”
A stable dose, regular medical review, and counseling support usually tell more about recovery progress than how quickly someone stops medication.
Long-term treatment makes the most sense when it’s helping a person live differently. In practical terms, that means fewer cravings, less chaos, more consistency, and lower risk behavior. It doesn’t mean side effects should be ignored. It means those side effects have to be weighed against what untreated opioid use disorder often brings back.
For many people seeking addiction treatment in Dallas, the healthiest plan isn’t an ideological one. It’s a personalized one. Some patients do well with extended maintenance. Others eventually taper under close supervision. The right timeline depends on relapse history, mental health, daily stability, medical issues, and whether the person is building a recovery life strong enough to hold without medication support.
Navigating Long-Term Physical Side Effects
A patient may tell me, “I’m not craving opioids, I’m showing up for work, but my body just doesn’t feel right anymore.” That deserves a careful medical discussion. Long-term Suboxone can be life-saving, and it can also bring physical side effects that need attention instead of dismissal.

Hormonal and adrenal changes
One under-recognized issue is how extended opioid-based treatment can affect hormone regulation. In practice, this can show up as lower sex drive, fatigue that doesn’t improve with rest, reduced stamina, and a general sense that the body is running slower than it used to.
Patients often assume these symptoms mean stress, aging, depression, or poor sleep. Sometimes that is true. Sometimes Suboxone is part of the picture, especially after long-term use.
Common signs worth bringing up at a medication follow-up include:
- Lower libido: Interest in sex drops or relationships start feeling strained.
- Persistent fatigue: Sleep may be adequate, but energy stays low.
- Less motivation: Daily tasks feel harder than they should.
- Reduced physical endurance: Exercise recovery is slower and aches linger longer.
These symptoms are not a reason to stop medication on your own. They are a reason to ask for a proper review, which may include lab work, a dose discussion, and screening for depression, thyroid issues, or other medical causes. In Dallas-Fort Worth, the best outcomes usually come from treating the whole picture instead of blaming everything on one medication.
Gentle movement can still help while the cause is being sorted out. If stiffness and deconditioning have started to build up, simple routines that improve hip mobility can be a reasonable place to start because they are low-impact and manageable for many patients.
Dental problems that people often overlook
Dental side effects deserve much more attention than they usually get. Suboxone films and tablets dissolve in the mouth, and repeated exposure can contribute to dry mouth, irritation, enamel wear, and cavities over time.
I encourage patients to treat mouth symptoms early. Waiting until there is pain usually means the problem has already become more expensive and harder to fix.
A few practical steps help:
- Rinse with water after the medication dissolves: This helps clear residue.
- Wait before brushing: Brushing right away can be rough on softened enamel.
- Address dry mouth early: Hydration, sugar-free saliva support products, and dental guidance can make a real difference.
- Keep regular dental visits: Preventive care matters more here than many people realize.
If dental issues keep recurring, it is reasonable to ask whether the formulation, dosing routine, or oral care plan needs to change. This is one area where clear coordination between addiction treatment and routine dental care can save a patient a lot of trouble.
Everyday physical issues that still matter
Some long-term side effects are less dramatic but wear people down over months. Constipation, sweating, headaches, nausea, dry mouth, and sleep disruption can chip away at quality of life even when recovery is otherwise going well.
Here is the practical approach I usually recommend:
| Symptom | What often helps |
|---|---|
| Constipation | Hydration, fiber, regular movement, and early medical treatment before it becomes severe |
| Dry mouth | Water, oral care habits, and consistent dental follow-up |
| Sleep disruption | Reviewing dose timing, sleep habits, caffeine use, and mental health symptoms |
| Ongoing nausea | Taking medication as directed, reviewing meal timing, and checking for other medical causes |
Side effects like these should be handled as active treatment issues. A patient does not have to choose between uncontrolled symptoms and relapse risk. The better plan is to adjust care early, involve medical and mental health support when needed, and keep the recovery plan workable for real life in Dallas.
Understanding the Psychological and Emotional Impact
A patient in Dallas can be doing many things right. Taking Suboxone as prescribed, staying away from illicit opioids, showing up for work, rebuilding trust at home. Then they sit across from me and say, “I’m stable, but I don’t feel like myself.”
That concern deserves a careful clinical response.
When emotions feel flattened
Some people on long-term Suboxone describe emotional blunting. Joy feels muted. Grief feels distant. Motivation drops, even when life on paper is getting better. Others feel less numb and more irritable, detached, or mentally tired. Those patterns matter because they can affect relationships, work, and willingness to stay in treatment.
Research has raised similar concerns. A PLOS One study reported flattened affect and reduced awareness of emotional states in some long-term buprenorphine-treated patients. That does not mean Suboxone causes the same experience in every person. It does mean emotional changes should be taken seriously instead of dismissed as a personality issue or a failure in recovery.
I tell patients this often. Feeling emotionally dulled is not a moral problem. It is a treatment issue.
The hard part is that emotional blunting has more than one possible cause. A dose may need review. Depression may be surfacing now that opioid use has stopped. Trauma symptoms may become clearer in early or sustained recovery. Sleep problems, chronic stress, grief, and other medications can all affect mood too. In some cases, it is a mix of several factors.
Why mental health care needs to stay connected to MAT
This is one reason integrated care matters so much in Dallas-Fort Worth. Opioid use disorder rarely shows up alone. Many patients also live with anxiety, depression, PTSD, panic symptoms, or bipolar-spectrum illness. If those conditions are left untreated, it becomes hard to tell whether Suboxone is the full problem, part of the problem, or protecting recovery while another condition is going untreated.
A short medication visit usually is not enough to sort that out well.
The better approach is coordinated care. A prescriber reviews dose, timing, side effects, and other medications. A therapist looks for trauma triggers, grief, isolation, and changes in functioning. If needed, psychiatric care helps clarify whether there is a co-occurring mood disorder that needs direct treatment. That kind of combined support gives patients a far better chance of feeling stable and emotionally present, not just opioid-free.
Families often notice the shift first. They may say their loved one seems calm but distant, physically present but checked out. That outside perspective can be useful, especially when the patient has trouble putting the change into words.
What to watch for over time
These are the signs I encourage patients and families to monitor:
- Loss of interest in relationships, hobbies, or goals that used to matter
- Feeling flat, numb, or disconnected for weeks at a time
- Ongoing sadness, hopelessness, or guilt
- Irritability that seems out of proportion to daily stress
- Isolation, avoidance, or trouble staying engaged in counseling
- Thoughts of self-harm or suicide, which require urgent professional help
Those symptoms do not automatically mean Suboxone is the wrong medication. They do mean the treatment plan needs review.
Sometimes the answer is a dose adjustment. Sometimes it is trauma therapy, depression treatment, or better sleep support. Sometimes a patient needs to revisit whether another medication approach fits better. If that discussion comes up, it helps to understand the difference between methadone and Suboxone in the context of your history, relapse risk, mental health needs, and daily life.
Patients tend to do best when they do not wait until numbness turns into disengagement. Early conversations can prevent a slow slide into missed appointments, relationship strain, and relapse risk. At Tru Dallas, that means looking at the full picture, medication, mood, trauma history, support system, and day-to-day functioning, so treatment remains livable over the long term.
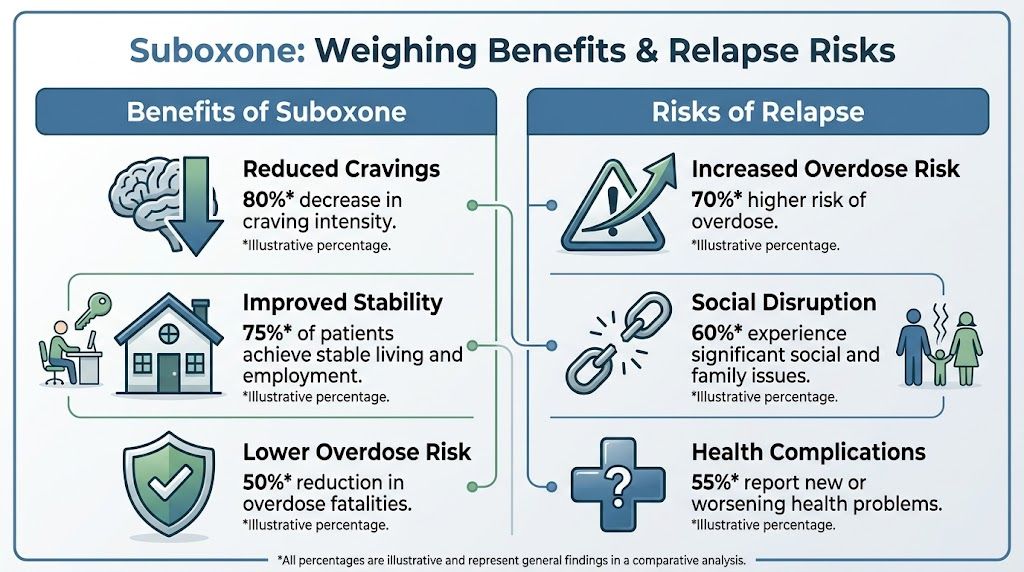
Suboxone's Benefits vs Risks of Relapse
Long-term side effects matter. They should be monitored seriously. But the decision to stay on Suboxone or taper off shouldn’t be made in a vacuum. It has to be measured against the risk of returning to untreated opioid use disorder.
That comparison changes the conversation.
What the health outcome data shows
A peer-reviewed analysis available through PMC on extended buprenorphine treatment outcomes found that patients who continued buprenorphine for at least 15 months had a 173% reduction in overdose events, a 52% reduction in all-cause inpatient hospital admissions, and a 26% reduction in emergency department visits compared with patients who stopped earlier.
Those aren’t small differences. They represent fewer overdoses, fewer medical emergencies, and fewer destabilizing crises. For many patients, the side effects of supervised treatment are manageable. Relapse often is not.
Some people considering long-term MAT also want to understand how other medication options compare. A useful starting point is this explanation of the difference between methadone and Suboxone, especially for patients discussing which path fits their history and daily routine.
The right treatment decision usually isn’t the one with zero downsides. It’s the one with the lowest overall risk and the highest chance of keeping someone alive, stable, and engaged in recovery.
Risk Comparison Long-Term Suboxone vs Untreated Opioid Use Disorder
| Risk Area | Long-Term Suboxone Use with Medical Supervision | Untreated Opioid Use Disorder Relapse |
|---|---|---|
| Overdose | Reduced risk with continued treatment, based on better health outcomes in extended buprenorphine care | High and often unpredictable risk, especially with fentanyl exposure |
| Hospital use | Lower inpatient and emergency utilization when treatment continues | More acute care episodes and instability |
| Cravings and withdrawal | Usually controlled enough to support daily functioning | Often return quickly and drive compulsive opioid use |
| Daily routine | Can support structure, work, appointments, and family involvement | Daily life often becomes organized around use, withdrawal, or recovery from use |
| Side effects | Real and sometimes significant, but medically reviewable | Medical, psychiatric, legal, and social harms usually expand over time |
This is why “just get off everything” can be dangerous advice. It sounds clean and simple, but addiction rarely behaves in a clean and simple way. If a patient is experiencing long-term Suboxone issues, the response should be a better treatment plan, not automatic discontinuation.
For many people in Dallas detox and rehab settings, the practical question is whether the current MAT plan is optimized. If side effects are becoming disruptive, that may mean dose review, therapy support, dental care, hormone evaluation, or eventually a carefully supervised taper. It doesn’t automatically mean the medication has stopped being useful.
How to Manage Side Effects and Improve Your Quality of Life
A common Dallas scenario looks like this. Someone is staying off illicit opioids, showing up for work, and doing many things right, but they are exhausted, their mouth feels dry all the time, intimacy has changed, or they feel emotionally flat. Those problems are treatable. They should not be carried alone until frustration turns into a risky decision.
The goal is to make treatment more livable while protecting recovery. In practice, that usually means tightening the plan around the medication instead of fighting with it in private.
Work with your prescriber in a precise way
Do not change your dose on your own. Taking extra medication, skipping doses, changing the time each day, or starting a self-directed taper can make side effects harder to interpret and cravings harder to control.
Specific details help your clinician make better decisions. Keep a short record for a couple of weeks and bring it to your appointment.
A useful review includes:
- Dose timing: Do symptoms show up right after dosing, in the afternoon, or all day?
- Mouth and teeth changes: Dry mouth, sensitivity, gum irritation, bad taste, or pain after films or tablets
- Mood and motivation: Emotional blunting, irritability, anxiety, low interest, or trouble concentrating
- Hormone and sexual symptoms: Lower libido, fatigue, weakness, erectile problems, or menstrual changes
- Sleep and bowel patterns: Insomnia, oversleeping, constipation, or nausea
A vague report can start the conversation. A specific report changes the treatment plan.
Reduce side effects with practical daily steps
Some long-term problems respond well to simple habits done consistently.
For dental protection, rinse your mouth with water after the medication dissolves and wait before brushing if your dentist has advised that approach. Stay current with dental cleanings. If dry mouth is persistent, ask about saliva-supporting products, sugar-free gum, hydration strategies, and whether the formulation or dosing routine should be reviewed. Dental discomfort is easy to minimize until it becomes expensive and painful.
Mental health support matters just as much. I often see patients assume every low mood or flat feeling is caused by Suboxone, when the fuller picture includes depression, trauma, grief, panic, or chronic stress. Good treatment sorts those issues apart instead of guessing. If you want a clearer sense of what counseling can look like, a guide to finding support through counselling can help you frame the right questions before you connect with care locally.
Quality of life also improves when the basics are protected:
- Sleep schedule: Keep the same wake time as often as possible
- Hydration and meals: Poor intake can worsen fatigue, nausea, and constipation
- Movement: Walking, stretching, or light exercise can help mood and bowel regularity
- Therapy follow-through: Continue counseling even after opioid use has stopped
- Medical follow-up: Ask for lab work or specialist review if symptoms suggest hormonal, metabolic, or psychiatric issues
Integrated care makes a real difference for DFW residents. If Suboxone is helping but side effects are building up, a program that can coordinate medication management, therapy, psychiatric support, and recovery planning is often the safest next step. For people looking for Suboxone treatment options in Dallas with ongoing clinical support, that level of follow-up can make treatment easier to stay with.
Know when to ask for help quickly
Some symptoms should be reviewed soon, especially if they are new or getting worse.
Call your clinician if you notice:
- Major fatigue or weakness that affects work, driving, parenting, or daily tasks
- Depression, emotional numbness, or suicidal thoughts
- Rapid dental decline, swelling, broken teeth, or persistent mouth pain
- Sexual or hormonal changes that are affecting relationships or functioning
- Cravings, isolation, dishonesty about medication use, or thoughts of returning to opioids
Some patients do decide to taper later. That can be appropriate. The timing matters. The safest tapers usually happen when housing, mental health, sleep, support systems, and relapse prevention are stable enough to carry the stress of dose reduction.
Long-term Suboxone care works best when the plan stays flexible and honest. If something feels off, say it early. In a strong treatment setting, side effects are not a reason to give up. They are a reason to adjust the care.
Find Your Path Forward at Tru Dallas Detox & Recovery Center
Long-term Suboxone use doesn’t need to be viewed as either a miracle or a mistake. It’s a medical treatment with clear benefits, real trade-offs, and a strong need for monitoring. For many patients, the medication remains protective. For others, the dose, formulation, mental health support, or long-range plan needs refinement.
What should never happen is silent suffering.
Hormonal changes, low energy, emotional flattening, dental problems, and treatment fatigue can all push a person toward disengagement if no one is paying attention. That’s a serious issue because Briarwood Detox’s discussion of long-term Suboxone maintenance risks notes that untreated hormonal side effects such as hypogonadism can double the risk of treatment dropout. That same discussion emphasizes that integrating specialized care, including endocrinology support and dual-diagnosis therapy, improves retention and supports sustained recovery.
That kind of coordinated care matters in practice. Patients in Dallas, Euless, Fort Worth, Arlington, and across DFW often need more than a prescription refill. They need a program that can look at the whole picture, including opioid recovery, psychiatric symptoms, medication side effects, family stress, relapse risk, and the practical next step.
For someone trying to decide what level of support fits, reviewing options for Suboxone treatment near Dallas can clarify what thorough care should look like. The most effective treatment plans usually include medical supervision, therapy, relapse prevention work, and follow-up that continues after the initial crisis has passed.
A patient who’s asking about suboxone side effects long term is usually not failing. More often, that patient is paying attention. That’s a strength. It means recovery has moved into a more thoughtful phase where health, function, and quality of life matter just as much as abstinence from illicit opioids.
The right next move is a professional review, not guesswork. With proper support, many long-term side effects can be managed, and treatment can become more comfortable, safer, and more sustainable.
If you or someone you love is struggling with long-term Suboxone side effects, relapse risk, or questions about medication-assisted treatment, Tru Dallas Detox & Recovery Center offers confidential, personalized support for people across Dallas-Fort Worth. The team provides medically supervised detox, MAT, dual diagnosis care, and ongoing treatment planning from its Euless facility. Reach out today to ask questions, verify PPO insurance, and find a safe path forward.