
Severe PTSD rarely stays contained to one part of life. It can show up in sleep, work, relationships, driving across Dallas traffic, walking into crowded stores, or trying to make it through a normal evening without feeling on edge. Some people live in a constant state of alert. Others feel numb, disconnected, or trapped by intrusive memories they can’t shut off.
That kind of suffering often leads people to try to manage alone for far too long. They may push through therapy that doesn’t feel like enough, miss appointments because symptoms spike, or rely on alcohol or drugs to blunt panic, nightmares, and agitation. By the time they start searching for ptsd inpatient treatment, daily life may already feel unmanageable.
Inpatient treatment is not a punishment and it isn’t a sign of failure. It’s a protected clinical setting built for safety, stabilization, and focused recovery. For people whose symptoms are severe, unpredictable, or tangled up with substance use, a residential level of care can create the calm needed to begin real healing. Instead of trying to recover in the same environment that keeps triggering the nervous system, inpatient care offers structure, supervision, and a clear plan.
Table of Contents
- What Is PTSD Inpatient Treatment
- Key Therapies in a Residential PTSD Program
- Inpatient vs Outpatient Care for PTSD in Dallas
- Treating PTSD and Substance Use Together in Dallas
- What to Expect A Typical PTSD Inpatient Program
- How to Start PTSD Inpatient Treatment in Dallas
- Frequently Asked Questions About Residential PTSD Care
What Is PTSD Inpatient Treatment
A Dallas resident may look stable from the outside, then spend the night cycling through nightmares, panic, drinking to calm down, and promises to quit in the morning. By the time they reach treatment, the problem is often larger than PTSD alone. They are trying to survive trauma symptoms and the fallout of using alcohol or drugs to blunt them.
PTSD inpatient treatment is residential care for people who need a protected, structured setting to regain stability before deeper trauma work can hold. The goal is practical. Keep the person safe, reduce daily chaos, and build enough physical and emotional steadiness for treatment to start working.
That structure matters. Inpatient care removes a lot of the pressure that keeps symptoms active in the community, such as access to substances, conflict at home, poor sleep, and constant exposure to triggers. For patients with severe hypervigilance, dissociation, self-harm risk, or substance use that complicates trauma treatment, a residential setting can provide the level of observation and support that outpatient care often cannot.

Who usually needs this level of care
This level of care is usually appropriate when PTSD has started to overrun daily life or when treatment keeps stalling because the person cannot stay regulated outside a controlled setting.
Common examples include:
- PTSD symptoms that disrupt basic functioning, including sleep, work, parenting, eating, or leaving the house
- Failed outpatient attempts because the person becomes overwhelmed between sessions or keeps dropping out
- PTSD with substance use when alcohol or drugs are being used to manage flashbacks, fear, agitation, or insomnia
- Safety concerns such as impulsive behavior, severe emotional swings, or symptoms that need close monitoring
In clinical practice, one rule helps. If someone cannot reliably stay safe, stay sober, or participate in treatment while living at home, inpatient care deserves serious consideration.
What inpatient treatment is trying to accomplish
Residential treatment gives patients a chance to get out of survival mode. That does not mean progress is fast or easy. It means the environment supports the work instead of fighting it.
For many people in Dallas-Fort Worth, the overlooked issue is dual diagnosis. PTSD and substance use often reinforce each other. Trauma symptoms drive the urge to numb out. Substance use then worsens sleep, anxiety, depression, irritability, and treatment dropout. Treating only one side of that cycle usually leads to relapse of symptoms, relapse of use, or both. A strong inpatient program addresses both conditions at the same time.
The core goals are clear:
| Goal | Why it matters |
|---|---|
| Safety | Staff can respond quickly when symptoms escalate or cravings increase. |
| Stabilization | Sleep, medication needs, withdrawal concerns, and daily routines have to settle before therapy can be effective. |
| Integrated treatment planning | PTSD and substance use are treated together so one problem does not keep reactivating the other. |
| Foundation-building | Patients begin evidence-based care and leave with a realistic next-step plan. |
What inpatient treatment often includes
People usually arrive worried that residential PTSD care means being pushed into trauma details before they are ready. Good programs do not work that way. Early treatment often focuses on stabilization, emotional regulation, substance use assessment, medication review if needed, and helping the nervous system slow down enough for real therapy to begin.
Trauma therapies may include trauma-focused CBT, EMDR, or Prolonged Exposure, but timing matters. In a dual-diagnosis setting, clinicians also have to watch for withdrawal, cravings, avoidance, and the ways substance use can interfere with memory, sleep, and emotional tolerance. That is one reason inpatient treatment can succeed after outpatient treatment has failed. The patient is not trying to manage trauma therapy, sobriety, and daily life all at once, without support.
The point is not to force disclosure. The point is to help patients become steady enough that trauma no longer controls every decision.
Key Therapies in a Residential PTSD Program
Residential PTSD care works best when treatment is structured, evidence-based, and delivered in a setting that can support patients through difficult moments without losing momentum.

A large veteran cohort study involving 10,832 people in residential PTSD programs found that symptom trajectories differed across patients, but most improved and many still needed follow-up care to maintain gains. The same source notes that trauma-focused inpatient therapies such as CBT and EMDR can produce response rates as high as 85%, full remission in 40% of patients, and that combining DBT with Prolonged Exposure reached 91% efficacy in VA settings. It also notes a 20% dropout rate, which is a useful reminder that treatment needs strong support and continuity, not just a good protocol (VA residential PTSD treatment findings).
Cognitive Processing Therapy and trauma-focused CBT
These approaches target the beliefs trauma can leave behind. Common examples include “I’m never safe,” “It was all my fault,” or “If I let my guard down, something bad will happen.”
In residential care, clinicians can catch those thoughts in real time. If a patient has a rough group session, a flashback at night, or a surge of shame after a phone call home, staff can use that moment therapeutically. That’s harder to do when care is limited to one appointment a week.
Inpatient advantage: the patient doesn’t have to figure out emotional recovery alone between sessions.
Outpatient limitation: the work may get interrupted by missed sessions, substance use, unstable sleep, or unsafe home dynamics.
For readers trying to build practical coping tools between therapy sessions, this guide on how to regulate emotions can be a useful companion resource. It won’t replace trauma treatment, but it can help people understand what emotional regulation looks like in daily life.
EMDR in a residential setting
EMDR often helps patients whose trauma memories feel stuck in the nervous system rather than fully processed. The memory may be old, but the body still reacts as if the threat is current.
A residential environment supports EMDR because the patient has somewhere to land afterward. There’s time to decompress, talk with staff, attend a grounding group, and follow a stable evening routine. That containment matters.
Some patients don’t need more insight first. They need enough safety and structure for the brain to process what it already knows.
Prolonged Exposure and the role of avoidance
Avoidance is one of the strongest engines of PTSD. People avoid memories, places, conversations, sleep, intimacy, and sometimes sobriety itself because all of it can feel too activating.
Prolonged Exposure works by helping the patient face trauma-related material in a planned, measured way. The goal is not distress for its own sake. The goal is learning that a memory can be revisited without total collapse, and that fear can rise and fall without dictating every choice.
Here’s where residential care often solves a practical problem:
- Problem in outpatient care: the patient leaves an exposure session and returns immediately to a chaotic home, easy substance access, or total isolation.
- Solution in inpatient care: staff can monitor the aftermath, adjust pacing, reinforce skills, and keep treatment moving.
Therapy works better when the setting is trauma-informed
A residential program can’t rely on therapy names alone. The environment also matters. Staff tone, boundaries, predictability, and clinical coordination all shape whether trauma treatment feels safe enough to continue.
A deeper discussion of that framework appears in this resource on trauma-informed care. It’s especially relevant when a patient has both PTSD and addiction, because shame and fear can derail treatment if the setting feels harsh or disorganized.
Inpatient vs Outpatient Care for PTSD in Dallas
A Dallas parent makes it through the workday, white-knuckles the drive home, pours a drink before dinner, and tells themselves they can hold it together until the next therapy appointment. By the end of the week, sleep is gone, irritability is up, and one trigger turns into a blowup, a binge, or a night of not feeling safe. That patient does not need a vague promise of “more support.” They need the right level of care.
Choosing between inpatient and outpatient treatment depends on function, safety, and whether the person can stay engaged in care without falling apart between sessions. Some people do well living at home and attending treatment several times a week. Others keep relapsing, dissociating, isolating, or spiraling after sessions because the setting around them is too unstable.
The decision usually comes down to what happens between sessions
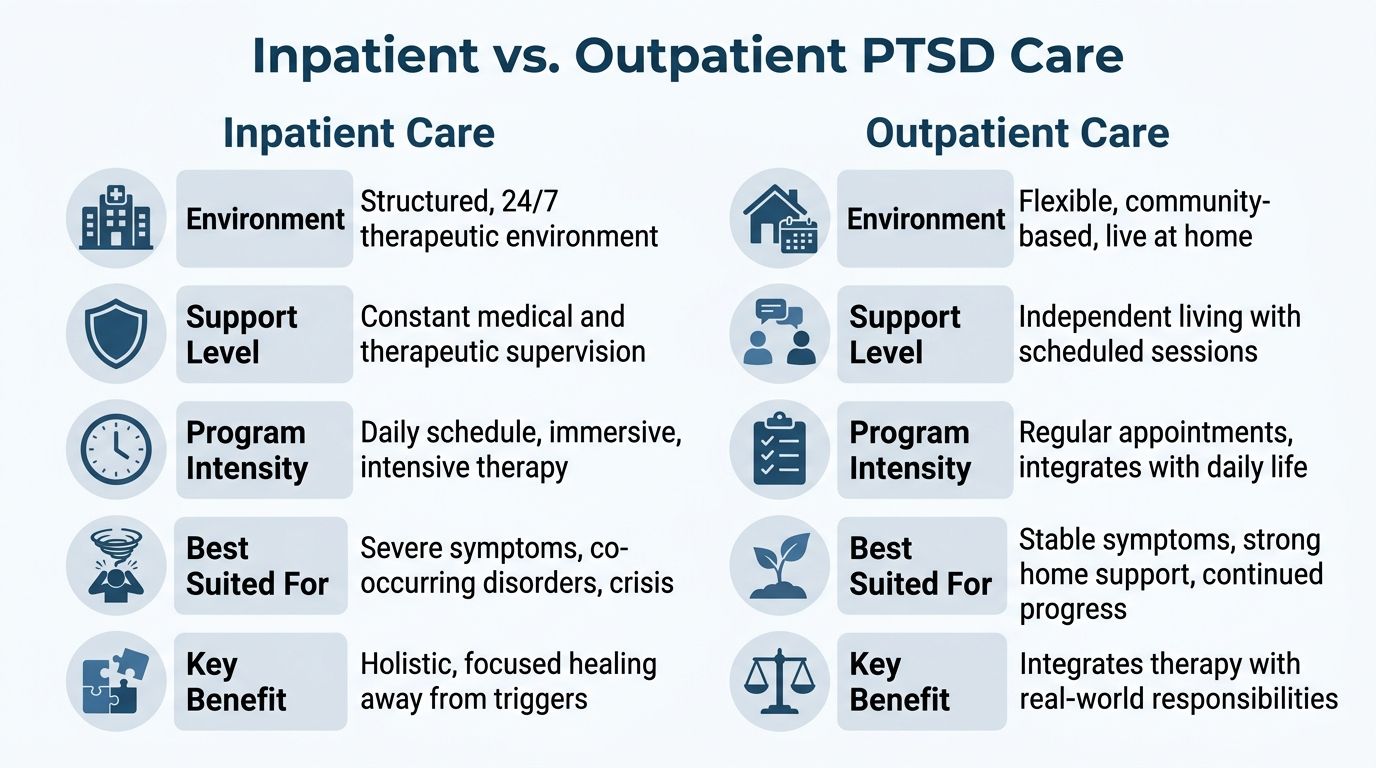
Here is the practical difference:
| Care level | Best fit | Main limitation |
|---|---|---|
| Inpatient | Severe PTSD symptoms, unstable sobriety, recent crisis behavior, major sleep disruption, or need for medical and psychiatric oversight | Requires time away from work, home, and daily routines |
| Outpatient | Symptoms are more contained, the home environment is dependable, and the person can use coping skills outside sessions | Triggers, cravings, and family stress can interrupt progress quickly |
I tell families to pay close attention to pattern, not intention. A patient may sincerely want recovery and still be unable to maintain it in an outpatient setting. If panic spikes after therapy, alcohol is easy to get, medications are inconsistent, and no one is monitoring safety at night, weekly care may be too thin for the severity of the problem.
PTSD with substance use changes the level-of-care decision
This is especially true in Dallas-Fort Worth, where people often try to keep working, parenting, and managing legal or relationship stress while PTSD and substance use feed each other in the background. Treating only the trauma or only the addiction often leads to the same cycle. Symptoms ease briefly, then the untreated half of the problem pulls the person backward.
Inpatient care can interrupt that cycle because the treatment team can address both conditions at the same time. That means managing cravings, tracking mood and sleep, adjusting medications carefully, and helping the patient recover after a difficult trauma session without immediate access to substances. Outpatient care can also treat both, but it works best when the person already has some stability, reliable transportation, and a home setting that does not constantly reactivate symptoms.
For patients who are stable enough to live at home but still need several therapy contacts each week, a trauma-focused intensive outpatient program may be the better fit.
Dallas-specific realities matter
Dallas patients are often trying to recover in the middle of long commutes, family pressure, unpredictable housing, and easy access to alcohol or drugs. Those factors are not side issues. They directly affect whether a person can follow through with treatment.
Inpatient care is often the better choice when any of the following are true:
- PTSD symptoms lead to repeated shutdown, rage, panic, or dissociation
- Substance use keeps returning after attempts at outpatient treatment
- The home environment is chaotic, unsafe, or filled with triggers
- Sleep is so poor that judgment and emotional control are falling apart
- The patient needs close medication monitoring or withdrawal support
- Trauma therapy has started before, but the patient could not stay regulated afterward
The better question is simple. What setting gives this person the best chance to stabilize, stay sober, and continue trauma treatment long enough for it to work?
Treating PTSD and Substance Use Together in Dallas
Many people with PTSD don’t start using substances because they want to get high. They start because they want relief. They want sleep. They want the shaking to stop. They want to get through a family gathering, a nightmare-filled night, or a flood of intrusive memories without feeling like they’re breaking apart.
That pattern is common enough that it should never surprise a treatment team. In 2023, Trauma Recovery Centers affiliated with the National Alliance of Trauma Recovery Centers served 11,929 survivors, and among their clients, 54% had a dual diagnosis, 49% had depression, and 22% had a substance use disorder including alcohol. The same report found 76% had PTSD diagnoses and 24% expressed suicidal ideation during treatment, which shows how severe and layered these cases can be. The data appears in the 2023 annual TRC data survey report.
Why one-condition treatment often falls apart
A patient enters rehab for alcohol, completes detox, and starts feeling physically better. Then nightmares worsen, shame surfaces, and hypervigilance returns. Without trauma treatment, the old reason for drinking is still intact.
Another patient starts trauma therapy while using opioids or benzodiazepines to suppress panic. Sessions become inconsistent. Emotional processing gets blunted or destabilized. The trauma work stalls.
This is why separate treatment tracks often create separate failures.
What a typical day may look like
A dual diagnosis residential program usually blends psychiatric care, addiction treatment, and trauma therapy into one coordinated schedule.
A day might include:
- Morning check-in with nursing or clinical staff to review sleep, cravings, mood, and medication effects
- Structured therapy groups focused on coping skills, relapse prevention, grounding, or psychoeducation
- Individual sessions where the therapist works on trauma symptoms, substance use patterns, and treatment goals together
- Medical monitoring when detox, medication-assisted treatment, or psychiatric medication adjustments are part of care
- Evening routine that supports sleep, emotional decompression, and safer transitions after a demanding therapy day
The key is coordination. Addiction staff and trauma clinicians can’t work like separate departments that barely speak to each other. The treatment plan has to reflect one interconnected problem.
What the first week often focuses on
The early phase is rarely about diving straight into the deepest trauma material. First, the team looks for stabilization points.
That usually means:
- Reducing immediate risk such as withdrawal problems, unsafe impulses, or severe agitation
- Restoring basic function through food, hydration, medication review, sleep support, and routine
- Building trust so the patient can engage treatment without feeling pushed too fast
A patient who is still withdrawing, sleeping two hours a night, and fighting panic all day usually needs stabilization before intensive trauma processing.
When care is integrated, patients don’t have to choose whether today’s “real problem” is PTSD or addiction. The program addresses both. For those searching for treatment that’s built around co-occurring conditions, this overview of dual diagnosis rehab explains how that model works in practice.
What to Expect A Typical PTSD Inpatient Program
Unknowns keep many people from getting help. They worry about losing control, being judged, or walking into a rigid environment they don’t understand. A good residential program reduces that uncertainty by making the process structured and predictable.
A common residential PTSD program lasts 30 to 45 days, which gives clinicians time to stabilize acute symptoms, begin evidence-based work such as CPT or PE, and prepare the patient for step-down care. That timeframe is described in this overview of evidence-based trauma-focused psychotherapies and residential treatment structure.
What the schedule usually includes
A residential day is active, but it shouldn’t feel chaotic.
Most programs include a mix of:
- Individual therapy to address trauma symptoms, treatment resistance, grief, shame, and recovery goals
- Group therapy for skill-building, psychoeducation, and connection with others facing similar struggles
- Medication management when psychiatric symptoms, sleep issues, cravings, or detox needs require monitoring
- Restorative activities such as mindfulness practice, movement, journaling, or quiet time for nervous system regulation
There is usually less idle time than people expect. That’s intentional. Structure lowers decision fatigue and reduces the chance that the day gets hijacked by avoidance or impulsive behavior.
Family involvement and aftercare planning
Family contact is often part of treatment, when it’s clinically appropriate and emotionally safe. That may involve education, boundary-setting, or joint sessions focused on communication and support.
Discharge planning should start early, not the week before leaving. The team typically works on outpatient referrals, relapse prevention, medication continuity, and practical housing or transportation needs before the residential stay ends.
A simple way to think about admissions
The admission process is often easier than people expect when it’s broken into steps.
Reach out for a confidential conversation
A brief call helps determine whether inpatient care is likely appropriate and whether urgent medical or psychiatric issues need immediate attention.Complete a clinical assessment
Staff gather history about trauma symptoms, substance use, current medications, safety concerns, and past treatment experiences.Review insurance and plan arrival
Many programs help verify benefits, explain next steps, and coordinate an admission timeline that feels manageable.
Sleep is one of the first systems to improve when treatment is working, but it often takes deliberate support. For readers who want practical habits to reinforce healthier rest, these sleep hygiene tips for optimal wellness can be a helpful supplement between clinical recommendations.
How to Start PTSD Inpatient Treatment in Dallas
Starting treatment is usually hardest before the first call. Once contact is made, the process becomes much more concrete.
Step one is the confidential phone call
The first conversation should be straightforward. The admissions team needs to know what symptoms are happening now, whether alcohol or drugs are involved, what medications the person is taking, and whether there are immediate safety concerns.
This is also the time to ask practical questions:
- Is inpatient treatment the right level of care
- Can the program treat trauma and substance use together
- What does the first day look like
- What should be brought to treatment
- How quickly can admission happen
Step two is a clinical assessment
A proper assessment looks beyond diagnosis labels. It should examine severity, relapse risk, current functioning, prior treatment history, family context, and whether the person needs detox, psychiatric stabilization, or both.
That matters because PTSD can present in very different ways. One person may be shut down and numb. Another may be panicked, sleepless, and impulsive. Another may look “high functioning” from the outside while barely holding life together.
Step three is insurance verification and admission planning
This step is where many people freeze. They assume insurance will be confusing, the logistics will be overwhelming, or they’ll have to sort everything out alone.
Strong programs make this easier. The team can often verify benefits, explain likely coverage, and walk the patient or family through timing, transportation, and required paperwork. For Dallas-Fort Worth residents, location also matters. A nearby program can make family coordination and step-down planning much smoother.
Treatment should feel clinically organized from the first call. If the admissions process is chaotic, patients often assume the care will be too.
For people in Dallas, Fort Worth, Euless, Irving, Arlington, and surrounding communities, the best next step is simple. Call, be honest about what’s happening, and let the clinical team determine the right level of care. Waiting for a “better time” rarely helps when PTSD and substance use are escalating together.
Frequently Asked Questions About Residential PTSD Care
Will treatment be private and confidential
Yes. Reputable programs protect patient privacy and handle personal health information according to confidentiality standards. That includes the initial phone call, the assessment process, and communication with family members.
If a family member wants updates, the patient usually needs to authorize that communication. This protects trust and gives the patient control over who is involved.
Can family be part of treatment
Often, yes. Family involvement can be very helpful when relatives want to support recovery but don’t understand trauma, addiction, or how to respond during a crisis.
That involvement may include educational sessions, family therapy, or discharge planning conversations. It should be guided by clinical judgment. Family participation helps most when it improves safety, boundaries, and follow-through after discharge.
What happens after inpatient treatment ends
Residential care is the beginning of stabilization, not the end of treatment. After discharge, many patients need step-down support such as outpatient therapy, psychiatric follow-up, recovery meetings, medication management, or sober living referrals.
A strong aftercare plan usually includes:
- Relapse prevention planning that names specific trauma triggers and substance use risks
- Follow-up therapy to continue trauma work after the residential stay
- Medication continuity so psychiatric care doesn’t abruptly stop
- Supportive housing or sober living referrals when the home environment is unstable
Does PTSD treatment help physical health too
It can help some areas, but the picture is mixed. The VA’s review of PTSD and physical health outcomes notes that while PTSD treatment can reduce psychological symptoms and may improve some health-related risks and self-reported health symptoms, effects on conditions such as cardiovascular disease are less clear. That’s one reason aftercare should include ongoing physical health monitoring, not just mental health follow-up.
What if outpatient care already failed
That doesn’t mean recovery is out of reach. It often means the level of care was too low for the severity of symptoms. Someone who couldn’t stabilize while living in the middle of triggers, insomnia, cravings, and daily stress may do much better in a residential setting with more structure and supervision.
The important move is not to repeat the same failed setup and hope for a different result.
If PTSD, alcohol use, drug use, or a dual diagnosis has made life feel unmanageable, Tru Dallas Detox & Recovery Center offers compassionate, structured care for adults across Dallas-Fort Worth. The team provides medically supervised detox, inpatient and outpatient treatment, dual diagnosis support, and help with insurance verification for most PPO plans. A confidential call can clarify options, answer urgent questions, and help determine the safest next step.