
A daughter notices that her father drinks the same way her grandfather did. A husband sees his wife reach for alcohol every night after stress, just like her mother once did. Someone in Uptown, Oak Cliff, Plano, or Arlington starts asking the same quiet question: can alcoholism be genetic, and if it runs in the family, what does that mean now?
That question usually carries fear with it. People aren't only asking about science. They're asking whether a family pattern can be changed, whether warning signs should be taken more seriously, and whether help should happen sooner instead of later.
The good news is that the answer isn't hopeless. Genetics do matter, but genetics don't make anyone powerless. Alcohol use disorder develops through a mix of inherited traits, life experiences, mental health, stress, trauma, and exposure to drinking environments. For families across Dallas and the wider DFW area, that distinction matters because it turns fear into action.
Some readers find it helpful to start with the basics of how genes work before thinking about addiction risk. A plain-language overview of the molecular biology of a gene can make the rest of this topic much easier to follow.
Table of Contents
- The Lingering Question Is Alcoholism In Your Genes
- Understanding the Genetic Link to Alcohol Use Disorder
- Common Genes That Influence How Your Body Processes Alcohol
- The Critical Interaction Between Your DNA and Your Life
- Navigating Your Family History and Personal Risk
- Personalized Recovery for Your Unique Blueprint at Tru Dallas
- Your Questions Answered
The Lingering Question Is Alcoholism In Your Genes
Families usually don't ask this question in a calm, academic moment. They ask it after a pattern becomes hard to ignore.
A son notices blackouts are starting to happen more often. A spouse sees promises to cut back keep breaking. A parent watches a college student come home from weekends in worse shape each time. When alcohol misuse already exists in the family tree, concern turns personal fast. People start wondering whether they inherited more than eye color and temperament.
That concern is valid. It also needs careful handling. Too many people swing to one of two extremes. They either assume alcohol problems are purely a matter of bad choices, or they assume family history means the outcome is already set. Neither view is accurate.
Practical rule: Family patterns should be treated as information, not a sentence.
The most useful way to think about inherited risk is this: a person may start out more vulnerable, but vulnerability isn't the same as inevitability. Some people inherit traits that affect how alcohol feels in the body or how strongly the brain responds to it. Others may have no obvious family history and still develop a serious problem because of trauma, stress, heavy social exposure, or untreated depression.
That distinction matters in real life across Dallas. Someone working long hours downtown, someone coping with grief in East Dallas, or someone managing anxiety in the Mid-Cities may all drink for different reasons, even if the biology underneath overlaps.
A concerned family member often wants a simple yes or no. Science gives a more honest answer. Alcohol use disorder can have a strong genetic component, but genes work together with environment. That means early support, better boundaries, mental health care, and addiction treatment in Dallas can still change the outcome in a meaningful way.
Understanding the Genetic Link to Alcohol Use Disorder
A lot of families reach this point in the conversation and want a clear answer. If alcohol use disorder shows up across generations, is that coincidence, learned behavior, or something inherited?

Research supports a real genetic contribution. According to the National Institute on Alcohol Abuse and Alcoholism overview on the genetics of alcohol use disorder, genes account for about 40-60% of the overall risk. That figure comes from studies comparing twins, adoptees, and families over time.
What heritability means in plain language
Heritability is easy to misunderstand. It does not mean a person is 50% destined to develop a drinking problem. It means inherited differences help explain why risk varies across a group of people.
A simple comparison helps. Genes work like the starting settings on a car. They can make the engine more sensitive, more reactive, or harder to regulate. But the road still matters. So does the driver. So do weather conditions, accidents, stress, and how often the car is pushed to its limit.
That is why two people can drink the same amount for a period of time and have very different outcomes.
Why adoption studies matter
Families often wonder whether alcohol problems are passed down through DNA or through what children see at home. Researchers have tried to separate those influences by studying adoptees. The American Academy of Child and Adolescent Psychiatry overview of substance use disorders notes that children of parents with alcohol use disorder are at a much higher risk, including when they are raised apart from their biological families.
That does not mean environment is secondary. It means both forces matter.
For some families, that finding brings relief. It gives a medical explanation for patterns that once looked like moral failure. For others, it stirs up fear. If risk is inherited, people worry the future is already written.
It is not.
Genes influence risk. They do not write the whole story.
Alcohol use disorder is polygenic. Many genes each make a small contribution. Some affect how rewarding alcohol feels. Some affect impulse control, stress reactivity, or the speed of alcohol metabolism. Some may overlap with traits linked to substance vulnerability more broadly. If you want context on those behavior patterns, this overview of addictive personality traits can help.
The part many articles miss is the interaction between biology and lived experience. A person can inherit some protection and still develop alcohol use disorder after repeated heavy drinking, trauma, chronic stress, or untreated anxiety or depression. A person with higher inherited risk can also lower that risk in a healthier environment with support, structure, therapy, and early treatment.
That point matters in real life across Dallas. A family history should prompt attention, not panic. It gives you a reason to watch for patterns earlier, take mental health symptoms seriously, and get help before occasional drinking turns into loss of control.
Genetic testing does not currently give families a full or reliable answer about who will develop alcohol use disorder. The useful question is usually not, "Do I have the gene?" The better question is, "Given my family history, stress load, trauma exposure, and current drinking pattern, what should I do next?"
That question leads people toward real help. And for many Dallas families, that is where change begins.
Common Genes That Influence How Your Body Processes Alcohol
A helpful place to start is the body's alcohol processing system. It works like a two-step assembly line. One set of enzymes turns alcohol into acetaldehyde, which is toxic. Another set clears that acetaldehyde out.
Metabolism genes can make drinking feel different
Two of the best-studied genes in that process are ADH1B and ALDH2. ADH1B affects how quickly alcohol is converted into acetaldehyde. ALDH2 affects how efficiently the body clears acetaldehyde afterward. The National Institute on Alcohol Abuse and Alcoholism explains that differences in these genes can change a person's physical response to alcohol, sometimes producing flushing, nausea, headache, or a racing heart that makes drinking much less appealing, as described in this NIAAA overview of alcohol metabolism.
That matters because risk is not only about willpower or family patterns. For some people, alcohol creates an immediate physical penalty. Their body sends a strong "stop" signal after only a small amount.
Families often find this reassuring and confusing at the same time. Reassuring, because it shows there are real biological differences in how alcohol feels. Confusing, because people assume a protective reaction means a person is safe from alcohol problems forever. It does not mean that. It means the body has one layer of resistance, and that layer can still be challenged by repeated exposure, social pressure, or drinking habits that build over time.
Some ancestry groups are more likely to carry certain variants, especially ALDH2 variants seen more often in people of East Asian descent. But these genes are not destiny, and they are not the whole story for any one person.
Brain signaling genes can raise vulnerability
Other genes influence alcohol response in a different way. They do less in the liver and more in the brain.
A commonly discussed example is GABRA2, a gene involved in the brain's GABA signaling system. Research summaries from major academic centers have linked some GABRA2 variants with higher susceptibility to alcohol problems, particularly in patterns that begin earlier and involve stronger reinforcement from drinking, according to this report on genetic risk factors associated with habitual heavy drinking.
Here is the practical meaning. One person may drink and mainly feel sick. Another may drink and feel unusually calm, relieved, or rewarded. Those are very different starting points, even before stress, trauma, grief, or mental health symptoms enter the picture.
| Gene | Primary Function | Possible Effect on Alcohol Use Disorder Risk |
|---|---|---|
| ADH1B | Helps convert alcohol into acetaldehyde | Some variants can make drinking less comfortable and may lower risk |
| ALDH2 | Helps clear acetaldehyde from the body | Some variants cause flushing and other unpleasant reactions that may discourage heavy drinking |
| GABRA2 | Affects brain signaling tied to calming and reward response | Some variants may increase vulnerability in certain people |
This is why families get mixed messages from what they observe at home. A relative who "never could hold their liquor" may have had a biological deterrent. A relative who seemed to relax instantly after a drink may have had a very different neurobiological response.
Neither pattern gives a full answer by itself. In real treatment work in Dallas, clinicians still need the full picture: current drinking, withdrawal risk, trauma history, anxiety or depression symptoms, sleep problems, and the home environment surrounding alcohol use.
The Critical Interaction Between Your DNA and Your Life
Genes matter. Life experience matters just as much, and sometimes more in day-to-day outcomes.
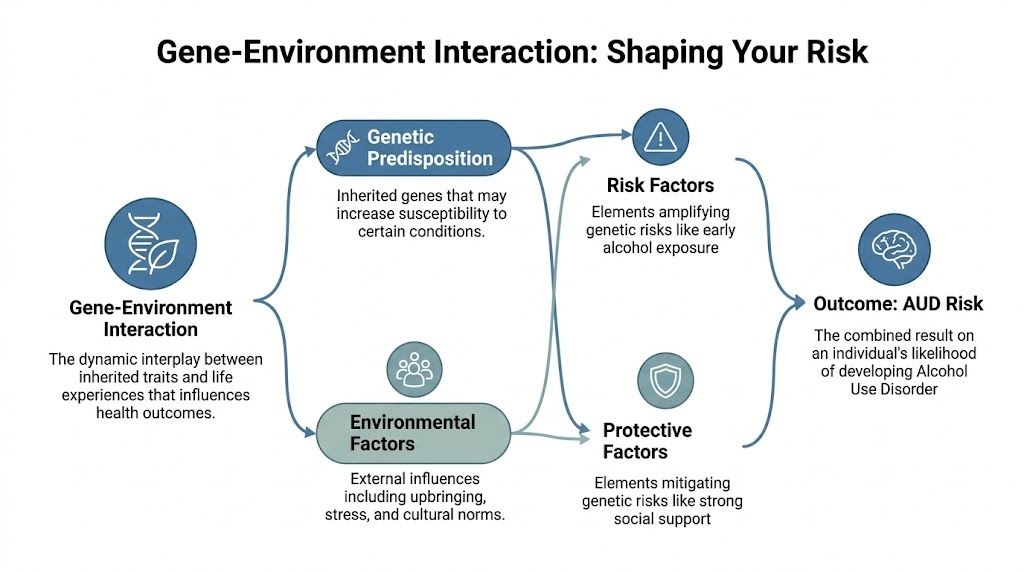
Protective genes don't cancel out real-world pressure
One of the most important findings in this field is that even protective genetic traits can be overridden by environment and social context. Research on ALDH2*2 notes that a protective allele can lose some of its power when social pressure is strong. The review states that individuals with the so-called protective allele might still drink when they're surrounded by friends who drink, and that environmental and social factors can override protective effects, as discussed in this PMC review of genes and alcohol dependence.
That idea clears up one of the most confusing family questions: "If someone had protective genes, how did they still end up here?"
The answer is that biology doesn't operate in a vacuum. A person may be less likely to enjoy alcohol at first, but repeated exposure, trauma, pressure to fit in, or a home environment centered around drinking can still change behavior over time. The same is true for someone with inherited risk. That risk may stay dormant for years until stress, loss, anxiety, or untreated PTSD push drinking from occasional to compulsive.
A genetic blueprint isn't the same thing as a life outcome.
This matters in Dallas because environment is never one single factor. It can include early family instability, relationship conflict, work stress, loneliness, social circles that normalize heavy drinking, or attempts to cope with depression and panic.
A supportive environment can reduce risk
The flip side is just as important. Supportive conditions can reduce the impact of inherited vulnerability.
A person with strong family history may never develop alcohol use disorder if certain protective conditions are present, such as:
- Stable relationships: People with reliable support are often less likely to use alcohol as their main coping tool.
- Early mental health care: Anxiety, trauma, and depression can drive drinking. Treating those conditions early can lower risk.
- Clear boundaries around alcohol: Families that recognize a pattern and respond early often reduce escalation.
- Low-risk social environments: Friend groups and work cultures strongly influence drinking behavior.
- Fast intervention after warning signs appear: Addressing binge drinking, blackouts, secrecy, or withdrawal symptoms early can change the trajectory.
A common example is the adult child of a parent with alcohol use disorder who decides in their early twenties to limit drinking, seek therapy for trauma, and avoid social scenes built around alcohol. That person may still carry inherited risk, but their daily choices and support systems reduce the chance that risk will become a disorder.
Another example runs in the opposite direction. Someone with no obvious family history begins drinking heavily after grief, isolation, and untreated anxiety. Over time, the environment creates the conditions for dependence even without a known inherited pattern.
This is why treatment that focuses only on the substance often misses a key element. For many people, a central clinical question isn't just "How much are they drinking?" It's "What is alcohol doing for them emotionally, and what keeps reactivating the cycle?"
Navigating Your Family History and Personal Risk
When alcohol problems run in a family, people often want a definitive answer about their own future. Medicine can't provide that. It can provide something more useful. It can identify risk, correct myths, and point toward practical next steps.
Family history is a warning sign, not a verdict
A family history of alcohol misuse should be taken seriously. It shouldn't be treated as fate.
Current research on polygenic risk makes that point clearly. Yale researchers reported that current polygenic risk scores explain only 1.3-1.9% of the variance in alcohol use disorder severity, and they emphasized that "no one is genetically 'destined' for alcoholism" because environment plays an equally important role and "accounted for the majority of the risk for alcohol use disorder", as described in this Yale summary on genetic, psychiatric, and environmental factors.
That means family history should push someone toward awareness, not resignation. A person who knows alcohol problems affect multiple relatives has strong reasons to monitor their own drinking truthfully, ask for help early, and take mood symptoms seriously.
Why genetic testing has real limits
Many readers get disappointed when they hope a DNA test can tell them whether they will or won't develop alcohol use disorder. Current testing can't do that with meaningful individual precision.
Some tests may identify specific variants related to alcohol metabolism. That can be interesting and, in some cases, clinically relevant. But a test result doesn't capture grief, trauma, marriage stress, job pressure, access to care, or the daily habits that shape behavior around alcohol.
For people who need a more immediate behavioral assessment instead of a broad genetic guess, a structured drug and alcohol evaluation can be a more practical starting point because it looks at actual patterns, consequences, and functioning.
Clinical takeaway: Family history is often more actionable than consumer genetic data because families already know the behavior pattern they are dealing with.
Practical ways families in Dallas can respond
Families in Dallas, Fort Worth, Euless, Irving, and surrounding DFW communities often ask what to do next when they recognize risk. The most helpful response is concrete and immediate.
- Track real warning signs: Blackouts, secret drinking, failed attempts to cut back, drinking to sleep, and withdrawal symptoms matter more than labels.
- Talk about family history openly: Silence often protects the addiction, not the family.
- Address mental health early: Trauma, anxiety, and depression can intensify alcohol misuse.
- Build a lower-risk lifestyle: Some people with strong family histories choose abstinence. Others set strict limits and monitor themselves closely.
- Get guidance before a crisis: Families don't have to wait for legal trouble, job loss, or a medical emergency.
When a loved one is already struggling, families may also benefit from practical guidance on how to help an alcoholic family member. The right next step isn't always confrontation. Often it's assessment, boundaries, and coordinated treatment planning.
Personalized Recovery for Your Unique Blueprint at Tru Dallas
The science around genetics matters most when it changes care. A person isn't treated effectively by focusing only on DNA or only on drinking behavior. Recovery works better when the full picture is addressed together.
Detox addresses the physical side safely
When alcohol dependence is already established, stopping suddenly can be dangerous. A medically supervised detox gives people a safer setting to manage withdrawal, stabilize physically, and begin treatment with clinical monitoring.
For anyone searching for a Dallas detox center or alcohol detox near the DFW area, that medical foundation matters. Alcohol withdrawal isn't a test of character. It's a medical event that needs the right level of support. Readers who need specifics on what that process involves can review this overview of alcohol detox.
In practical terms, detox handles the immediate crisis. It creates enough safety and clarity for the deeper work to begin.
Dual diagnosis care treats the drivers underneath
Many people with alcohol use disorder aren't only battling alcohol. They're also dealing with trauma, panic, depression, bipolar symptoms, chronic stress, or another substance. That's why treatment has to reach below the surface.
A personalized plan may include:
- Psychiatric evaluation: This helps identify whether anxiety, depression, trauma symptoms, or mood instability are fueling drinking.
- Individual therapy: One person may need trauma-focused work. Another may need relapse prevention and coping skills.
- Group counseling: Structured peer support can reduce isolation and shame.
- Medication-assisted support: For some patients, medication can help reduce cravings, stabilize mood, or support recovery.
- Family involvement: Family systems often need repair, education, and clearer boundaries.
That matters locally because many people seeking addiction treatment in Dallas are balancing work, parenting, relationships, and untreated mental health symptoms at the same time. The more complex the picture, the more important integrated care becomes.
Aftercare matters in the real world
A person doesn't recover in a vacuum. They recover in apartments, workplaces, families, and social circles that may still contain the same pressures that fed the disorder.
That's why discharge planning and aftercare aren't minor add-ons. They are where treatment gets tested. A strong plan may include outpatient follow-up, therapy, medication management, sober living recommendations, relapse prevention work, and family counseling.
For people across Dallas, Fort Worth, and the surrounding metroplex, the most effective treatment approach is one that respects both parts of the equation. Biology may shape vulnerability. Environment often shapes whether that vulnerability gets activated again.
Your Questions Answered
If alcoholism runs in a family, is developing it guaranteed
No. A family history points to higher susceptibility, not a fixed outcome. Researchers have found in adoption and family studies that biological relatives of people with alcohol problems face a meaningfully higher risk, even when they grow up in a different home environment, according to the National Institute on Alcohol Abuse and Alcoholism.
Genes work more like a loaded dice roll than a sentence. They can tilt the odds. They do not decide the final result. Daily stress, trauma, early exposure to alcohol, peer pressure, mental health symptoms, and access to support all help shape what happens next.
Can a DNA test tell someone whether they will become an alcoholic
No. Current DNA testing cannot tell one person, with real clinical certainty, whether they will develop alcohol use disorder.
That can feel confusing, especially when genetics clearly matter. The reason is that alcohol use disorder is not caused by one gene flipping on like a light switch. It involves many small genetic influences mixed with life experience. A test may show clues about alcohol metabolism or inherited vulnerability, but it does not measure grief, trauma, isolation, depression, or the drinking culture around someone. Those factors often decide whether risk stays quiet or becomes a serious problem.
For families in Dallas, that means genetic testing should never replace a full mental health and substance use assessment.
Why do some people with strong family histories never develop AUD
Protection can come from the environment as much as the genome. A person may have inherited risk, then grow up with structure, honest conversations about addiction, treatment for anxiety, and limited exposure to heavy drinking. Another person may have some genetic protection, then lose ground after trauma, chronic stress, or untreated depression.
That interaction matters. It explains why two siblings from the same family can have very different outcomes.
Some people avoid alcohol altogether because they know their history. Others get help early, before drinking becomes a primary coping tool. Supportive relationships, stable housing, trauma treatment, healthy routines, and clear boundaries can lower risk in real life.
When should a family in Dallas reach out for professional help
Reach out when alcohol starts changing the person or the home. Common warning signs include secrecy, repeated arguments, missed responsibilities, blackouts, risky behavior, withdrawal symptoms, worsening anxiety or depression, or repeated promises to cut back that do not last.
You do not need to wait for an arrest, job loss, or medical emergency.
Early care often gives families more choices, less chaos, and a better chance to address the full picture, including mental health, trauma, and the patterns around drinking that keep repeating.
When alcohol misuse starts to feel like a family pattern, waiting usually adds fear and confusion. Tru Dallas Detox & Recovery Center helps individuals and families across Dallas-Fort Worth take the next step with confidential guidance, medically supervised detox, dual diagnosis support, and personalized treatment planning. Reaching out to verify insurance, ask questions, or request an assessment can turn uncertainty into a clear plan for recovery.