
Most advice about an “addictive personality” gets the first step wrong. It treats addiction risk like a fixed identity, as if a person is born with one doomed type of mind.
That label sounds simple, but it often creates more fear than clarity. Families hear it and think, “So this was inevitable.” People who are struggling hear it and think, “So this is just who I am.” Neither conclusion is helpful.
A more accurate way to understand addictive personality traits is this. Some people carry a spectrum of risk factors that can make alcohol, drugs, or compulsive behaviors harder to resist and harder to stop once they start. Those traits are real. The label is the problem.
That distinction matters in Dallas, where many families are trying to decide whether a loved one needs a detox program, rehab, dual diagnosis care, or a professional assessment before things get worse. Clear language leads to better decisions. Stigma delays help.
Table of Contents
- Understanding Addiction Beyond a Simple Label
- The Myth of the Single Addictive Personality
- Key Traits and Behaviors That Increase Addiction Risk
- The Scientific Roots of Addiction Vulnerability
- Recognizing the Signs and Seeking Help in Dallas
- Personalized Treatment for Lasting Recovery at Tru Dallas
- Frequently Asked Questions About Addiction Risk
- If addiction runs in a family, is recovery still possible
- Can these traits change over time
- What is the first step for a family in Dallas
- Do addictive personality traits mean someone is a bad person
- Can someone need help even if life hasn't completely fallen apart
- Is detox enough by itself
- What if the loved one says they can stop anytime
Understanding Addiction Beyond a Simple Label
The phrase addictive personality traits keeps showing up because people are trying to explain a real pattern. Some individuals do seem more vulnerable to compulsive behavior, stronger cravings, and repeated relapses.
But vulnerability isn't the same thing as identity.
A person may be impulsive, highly sensitive to stress, drawn to intense experiences, or slow to think through consequences. Those patterns can increase addiction risk. They don't prove a person is broken, weak, or incapable of recovery.
That shift in language matters for families. When a spouse, parent, or adult child sees addiction as a character flaw, the conversation usually becomes moral. When they understand it as a mix of traits, biology, mental health, and environment, the conversation becomes practical.
A fixed label can trap a family in blame. A risk-based view opens the door to assessment, treatment, and change.
In the Dallas-Fort Worth area, this is often the moment when concern turns into action. A family stops asking, “Why can't this person just control it?” and starts asking better questions. What triggers the behavior? Is there co-occurring anxiety, depression, or trauma? Does the person need a Dallas detox center, residential care, outpatient support, or medication-assisted treatment?
Those are treatment questions, not judgment questions.
The most useful takeaway is simple. The old label is too crude. The outlook is more hopeful. Addiction risk usually comes from multiple interacting factors, and those factors can be assessed and treated.
The Myth of the Single Addictive Personality
The idea of one single addictive personality sounds neat, but real people don't work that way. Two individuals can both develop substance use problems for very different reasons.
One may be impulsive and thrill-seeking. Another may be anxious, isolated, and desperate for relief. Both can end up in the same dangerous cycle, but they didn't arrive there through the same route.
Why the label can cause harm
When people hear “addictive personality,” they often translate it into something harsh:
- Permanent identity: “This person will always be this way.”
- Personal failure: “This is just bad judgment.”
- Hopeless future: “Treatment probably won't help.”
- Family shame: “Something is wrong with this whole family.”
Those beliefs can delay care. They can also make someone hide substance use longer, especially in high-pressure settings like college, professional workplaces, or socially image-conscious communities around Dallas.
Shame tends to make addiction more secretive. Secretive addiction tends to get worse.
A better model than a single type
A more accurate model is a constellation of traits. Different traits can combine in different ways, much like ingredients in a recipe.
A simple comparison helps:
| Pattern | What it may look like | Where risk grows |
|---|---|---|
| Impulsive risk pattern | Fast decisions, weak brakes, thrill-seeking | Experimentation turns into repeated use |
| Distress relief pattern | Anxiety, sadness, overwhelm, emotional escape | Substances become coping tools |
| Social approval pattern | Strong need to fit in, fear of rejection | Peer environments shape ongoing use |
| Compulsive routine pattern | Repetition despite consequences | Habit becomes hard to interrupt |
This model is more humane because it leaves room for resilience. A person may have risk traits and still never develop an addiction. Another may have moderate risk but encounter severe stress, trauma, or easy access to substances and then spiral quickly.
Practical rule: Risk factors raise the odds. They don't erase choice, treatment response, or the possibility of long-term recovery.
The label also misses the fact that addiction can involve substances and behaviors. A person may struggle with alcohol, opioids, stimulant misuse, gambling, compulsive exercise, internet use, or several patterns at once. That doesn't point to one personality. It points to overlapping vulnerabilities.
Families in Dallas often feel relief when this becomes clear. If there isn't one fixed “type,” then treatment doesn't need to force every patient into the same mold. Effective addiction treatment in Dallas should look at the whole picture, including mental health, coping style, trauma history, daily structure, and relapse triggers.
That is far more useful than attaching a label and hoping it explains everything.
Key Traits and Behaviors That Increase Addiction Risk
Some traits show up again and again in people who struggle with substance use or compulsive behaviors. That doesn't mean every person with these traits will become addicted. It means these patterns can make risky behavior more likely and recovery more complicated if they aren't addressed directly.
Impulsivity and acting before thinking
Impulsivity is one of the clearest risk factors.
In plain language, it means the brain struggles to pause. A person feels an urge and acts before weighing the cost. That can show up as binge drinking after a stressful day, taking extra pills without thinking, driving under the influence, sudden spending, angry outbursts, or repeatedly breaking personal rules.
Research on impulsivity and addiction has linked this trait to dysregulation in the prefrontal cortex, the part of the brain involved in judgment and inhibition. The same research found stronger attentional bias toward substance cues in highly impulsive individuals, with effects up to r=0.48, and noted that DRD2 variants can make impulsive individuals 2 to 3 times more likely to develop addictions (PMC article on impulsivity and addiction).
That sounds technical, but its practical application is straightforward. The person's attention gets pulled toward the substance faster, and the ability to interrupt the urge is weaker.
Sensation-seeking and the chase for intensity
Some people are wired to seek novelty, speed, stimulation, or strong emotional highs. This is often called sensation-seeking.
It may look harmless at first. Constant need for excitement. Boredom with routine. Jumping from one intense experience to another. A tendency to say yes before thinking through the risk.
For one person, this might mean escalating alcohol use at parties. For another, it might mean mixing substances, chasing stronger highs, or moving from occasional use to more dangerous experimentation.
This trait can confuse families because the person may seem energetic, social, or charismatic. The deeper issue is that ordinary rewards may not feel satisfying enough for long.
Emotional volatility and stress sensitivity
Not everyone uses substances to feel more excitement. Many use them to feel less pain.
A person with high emotional reactivity may feel stress, rejection, guilt, loneliness, or conflict very intensely. When healthy coping skills are weak, alcohol or drugs can start to look like relief.
Examples include:
- Stress drinking: A person starts every evening saying they need something to “take the edge off.”
- Anxiety-driven misuse: Prescription medications are taken outside medical guidance to calm fear or tension.
- Conflict-triggered relapse: Arguments, breakups, or criticism quickly lead back to use.
This pattern is easy to miss because it may not look reckless on the surface. It can look quiet, private, and controlled until it suddenly isn't.
Low conscientiousness and weak follow-through
Conscientiousness refers to planning, self-discipline, reliability, and staying consistent with long-term goals. When it's low, people may struggle with routines that protect recovery.
That can look like missed appointments, half-finished commitments, poor sleep habits, unpaid bills, skipping medications, or repeated promises that collapse under pressure.
A person may want to stop using. The problem is that wanting recovery and organizing life around recovery are not the same skill.
A short list can help families spot the difference between a rough patch and a pattern of risk:
- Frequent short-term decisions: The person chooses immediate relief over long-term stability.
- Low frustration tolerance: Small setbacks lead to outsized reactions or impulsive use.
- Repeated rule-breaking: Limits are made and broken in quick cycles.
- Difficulty delaying gratification: Waiting feels unbearable, even when consequences are obvious.
Traits are not moral defects. They are patterns of emotion, attention, and behavior that treatment can target.
These traits also overlap. Someone can be both impulsive and highly anxious. Someone can crave stimulation but also use substances to numb emotional pain. That overlap is why a thorough assessment matters. Good care doesn't ask only, “What is the person using?” It also asks, “What function is the substance serving?”
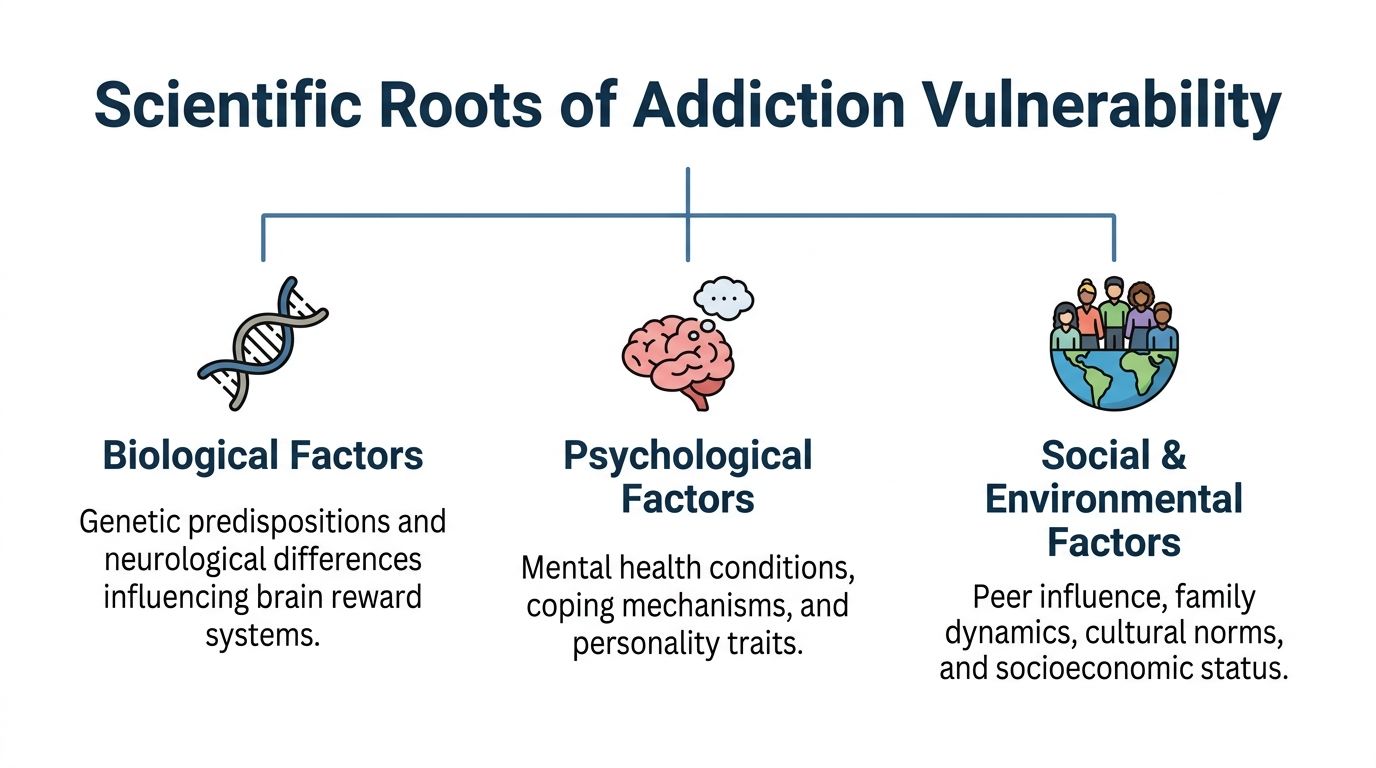
The Scientific Roots of Addiction Vulnerability
The most useful way to think about addiction risk is through three connected influences. Biology, psychology, and environment all matter. None tells the whole story alone.
Biology shapes risk but doesn't write destiny
Genetics play a major role in addiction vulnerability. Research estimates that 40% to 70% of an individual's vulnerability is heritable, and those inherited traits can include impulsivity and sensation-seeking linked to dopamine-related pathways (overview of heritability and addictive personality traits).
That doesn't mean a gene causes addiction in a simple, one-to-one way. It means some people begin life with a more sensitive reward system, weaker impulse control, or a stronger pull toward novelty and reinforcement.
For families, this can be clarifying. A strong family history may reflect shared biology as much as shared stress or shared exposure.
Psychology affects coping and reward
Mental and emotional patterns shape what a person does with that vulnerability.
If someone has untreated anxiety, depression, trauma reactions, or difficulty managing distress, substances can start to serve a psychological job. They may numb panic, mute shame, quiet intrusive memories, or create short bursts of confidence.
That is why skill-building matters. Resources that explain how habits form can be useful when families are trying to understand repetition, cues, and reward loops. A practical example is Mastering Habit Formation Psychology, which helps translate abstract behavior patterns into everyday terms.
For many patients, trauma is part of this picture. A trauma-informed approach changes how professionals interpret withdrawal, reactivity, avoidance, and distrust. Families who want to understand that treatment lens can review this explanation of trauma-informed care.
Environment can push risk higher or lower
The surrounding environment often decides whether a vulnerability stays manageable or becomes dangerous.
A few common examples:
- Peer exposure: Frequent substance use in a social circle can normalize risky behavior.
- Chronic stress: Financial pressure, family conflict, unstable housing, or burnout can increase the urge to escape.
- Early trauma: Painful experiences can shape coping patterns long before substance use starts.
- Isolation: People with weak social support often have fewer buffers when cravings rise.
This is why two siblings from the same family can have very different outcomes. Shared genetics don't guarantee shared behavior. Different friendships, stress levels, coping skills, and life events can steer risk in very different directions.
The question isn't whether addiction is biological or psychological or social. It's how those forces are interacting in one person's life right now.
That is also why treatment works best when it addresses more than the substance itself. Detox may stabilize the body. Therapy may build coping skills. Family work may reduce conflict. Ongoing structure may protect against relapse. Recovery becomes more durable when the full web of risk is treated, not just the visible symptom.
Recognizing the Signs and Seeking Help in Dallas
Families usually don't need a perfect diagnosis to know something is wrong. They need permission to trust what they're seeing.
A national meta-analysis found that 47% of U.S. adults experience signs of an addictive disorder annually, and among college students, up to 75% report at least one addictive behavior (American Addiction Centers overview of addictive personality traits). In the Dallas-Fort Worth area, that matters for parents of college students, spouses of working adults, and families watching prescription misuse develop into dependence.

What families often notice first
The earliest warning signs are often behavioral, not dramatic.
Common patterns include:
- Escalating secrecy: Hidden bottles, vague explanations, deleted messages, or defensiveness about simple questions.
- Mood changes: Irritability, anxiety, shutdown, agitation, or sudden emotional swings.
- Broken routines: Missed work, skipped classes, poor sleep, neglected hygiene, or loss of interest in normal responsibilities.
- Using despite consequences: The person keeps going after fights, legal trouble, health concerns, or clear damage to relationships.
- Withdrawal from support: Pulling away from family, healthy friends, hobbies, or structure.
Sometimes the family keeps waiting because the person is still functioning on the surface. They may still work, parent, or keep appointments. Functioning doesn't mean safe.
When to stop waiting
A practical rule helps. Concern becomes urgent when a pattern is repeated, escalating, and defended.
A family doesn't need to wait for rock bottom if they are seeing things like:
- substance use to manage every bad day
- repeated failed attempts to cut back
- mixing substances or taking more than intended
- lying about use, money, or whereabouts
- signs of withdrawal when the substance isn't available
If a family is changing its own behavior to manage someone else's substance use, the problem is already serious enough to evaluate.
For people in Dallas who aren't sure what level of care is needed, a starting point is a professional addiction assessment. That can clarify whether the person needs detox, residential rehab, outpatient treatment, dual diagnosis care, or a medical review for withdrawal risk. Local treatment options are available through this Dallas addiction treatment center.
The hardest part is often the first call. But uncertainty is not a reason to delay. When the signs are consistent, getting help is usually safer than waiting for a crisis to force the decision.
Personalized Treatment for Lasting Recovery at Tru Dallas
A person doesn't recover because someone handed over generic advice. Recovery gets stronger when treatment matches the actual drivers behind the addiction.
That matters with addictive personality traits because different risk patterns need different interventions. The person who uses impulsively may need stronger relapse interruption and structure. The person who uses to numb panic or grief may need deeper mental health treatment alongside addiction care.
Matching treatment to the person
Some traits respond especially well to targeted care. For example, high neuroticism and low conscientiousness are linked to higher addiction vulnerability, with meta-analyses reporting odds ratios of 1.8 to 2.5 for substance dependence. Trait-informed care also matters in treatment retention. One cited example is DBT, which can reduce rehab dropout by 35% in high-neuroticism patients (discussion of traits and DBT in addiction care).
In practice, personalized treatment often looks like this:
- Medical detox for physical dependence: Patients withdrawing from alcohol, opioids, or certain prescription drugs may need supervised stabilization before therapy can work well.
- Dual diagnosis treatment for emotional drivers: If anxiety, depression, bipolar disorder, or trauma symptoms are fueling use, both conditions need treatment together.
- DBT for distress and emotional reactivity: This can help people who feel overwhelmed fast and use substances to escape those states.
- CBT for impulsive thinking patterns: This helps patients slow down thoughts, challenge permission-giving beliefs, and build more realistic decision-making.
- MAT for opioid or alcohol use disorders: Medication-assisted treatment can reduce cravings and support stability while therapy addresses behavior and mindset.
A treatment overview is available at how treatment works at Tru Dallas.
Why continuity of care matters
Addiction rarely begins in one day, and recovery usually doesn't stabilize in one stage of care either.
A patient may start in detox, move into inpatient or outpatient treatment, continue with individual and group therapy, and then need a structured aftercare plan. That continued support matters because traits like poor follow-through, emotional reactivity, and cue-driven cravings don't disappear the moment substance use stops.
A strong plan often includes:
| Need | Helpful treatment response |
|---|---|
| High impulsivity | Structured schedule, coping rehearsal, relapse planning |
| Stress-triggered use | Therapy for emotional regulation and trigger mapping |
| Co-occurring mental health symptoms | Integrated psychiatric and addiction care |
| Weak daily structure | Routine-building, accountability, aftercare planning |
| Family conflict | Education, communication work, boundary-setting |
Good treatment doesn't just remove substances. It teaches the person how to live without needing them for relief, reward, or escape.
That is why families looking for a Dallas detox center or rehab program should pay attention to personalization, medical support, dual diagnosis care, and discharge planning. Lasting recovery depends on treating the person behind the pattern, not just the pattern itself.
Frequently Asked Questions About Addiction Risk
If addiction runs in a family, is recovery still possible
Yes. Family history can increase vulnerability, but it doesn't make addiction inevitable and it doesn't make treatment pointless.
A person may inherit sensitivity to reward, stress, or impulsive behavior. Recovery is still possible because treatment can change daily routines, coping skills, medication support, environmental exposure, and response to triggers. Risk is real. So is the ability to reduce it.
Can these traits change over time
They can.
Some traits soften with maturity, structure, therapy, and sobriety. Others may remain part of the person's temperament but become much more manageable. An impulsive person can learn to pause. A highly anxious person can learn distress tolerance. A disorganized person can build routines that protect recovery.
The goal isn't to create a new personality. It's to reduce the power those traits have over behavior.
What is the first step for a family in Dallas
The first step is usually a confidential assessment with a treatment professional who can evaluate substance use, withdrawal risk, mental health symptoms, and level of care needs.
Families don't need to prepare a perfect script. It helps to gather a few concrete examples:
- changes in use patterns
- failed attempts to stop
- recent consequences
- signs of withdrawal or instability
- mental health concerns that seem tied to use
That information gives the clinical team something real to work with.
Do addictive personality traits mean someone is a bad person
No.
These traits describe patterns of risk, not moral worth. A person may struggle with impulsivity, emotional pain, or compulsive behavior and still be caring, intelligent, responsible in other areas, and profoundly ashamed of what is happening.
Shame often blocks treatment. Understanding opens the door to treatment.
Can someone need help even if life hasn't completely fallen apart
Yes. Waiting for total collapse is dangerous.
Many people meet criteria for serious substance problems while still holding a job, attending school, or appearing functional to others. Early help can be less disruptive and safer than waiting for legal trouble, overdose, medical complications, or a psychiatric crisis.
Is detox enough by itself
Usually not.
Detox addresses the body's immediate dependence and withdrawal. It does not, by itself, resolve the emotional habits, thinking patterns, trauma responses, environmental triggers, or mental health symptoms that keep addiction going. For many people, detox is the beginning of treatment, not the whole treatment.
What if the loved one says they can stop anytime
That statement is common. The more useful question is whether they have.
If someone keeps promising to stop but repeatedly returns to the same behavior, the issue is no longer just intention. It is loss of control, poor coping, or both. That is exactly where professional treatment can help.
For families and individuals looking for a trusted next step, Tru Dallas Detox & Recovery Center offers medically supervised detox, evidence-based addiction treatment, dual diagnosis care, and ongoing recovery support for the Dallas-Fort Worth community. A confidential conversation can help clarify whether detox, rehab, or mental health treatment is needed, verify PPO insurance options, and make the first step feel manageable.